Retroperitoneal hemorrhage
The pathophysiology is unknown. Some hypothesize that occult vasculopathy and arteriosclerosis of the small vessels in the retroperitoneum may render them friable and therefore prone to rupture. This can be seen in minor trauma in sports and forceful vomiting or coughing. Spontaneous bleeding starts at the microvascular level, and large vessels become disrupted or stretched as the hematoma enlarges.
Retroperitoneal hemorrhage occurs in a variety of clinical circumstances, including spontaneous hemorrhage into a pre-existing benign adrenal cyst or bleeding from a left inferior phrenic artery, tumors of the adrenal gland and kidney, rupture of any blood vessel (most commonly infrarenal aorta); percutaneous interventions (such as cardiac catheterization), trauma, and polycythemia vera,
It is most commonly seen in association with patients with bleeding abnormalities, in HD patients and with anticoagulation therapy,. Risk is much greater with unfractionated heparin therapy than with warfarin. In most of the heparin patients studied, their coagulation parameters were in the therapeutic range.
Patients may present to the non acute area of the ED with back, lower abdominal or groin discomfort, Over time, this may progress to hemodynamic instability, and a fall in hemoglobin, Early identification is crucial to improving patient morbidity and mortality. Early symptoms depend on the location of the bleeding.
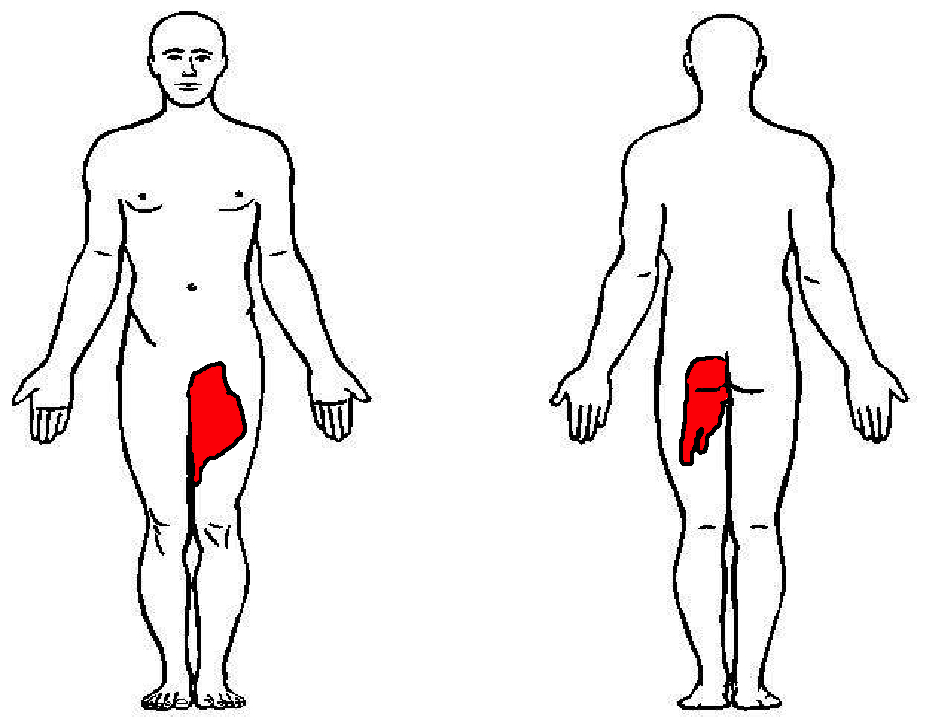
Hematoma near or within the iliopsoas muscle usually presents as femoral neuropathy (groin pain or leg weakness).
Femoral neuropathy caused by retroperitoneal hematoma can present with sudden onset severe pain in the affected groin and hip, with radiation to the anterior thigh and the lumbar region. This can easily be missed as the presentation is similar to a pulled msucle or strained hip/back. Iliopsoas muscle spasm often results in the characteristic flexion and external rotation of the hip, and any attempt to extend the hip will result in severe pain. Over time, pain and parasthesia in the antero-medial thigh and leg is seen.
Chan, Morales; et al., 2008. Int J Clin Pract.
%20copy%201.JPG)