{kind=link}
Screening Tool for Large Vessel Occlusion Strokes (LVOS)?
- Endovascular intervention for acute ischemic stroke from ICA or proximal MCA occlusion is a Level IA recommendation1.
- Identification of patients who may benefit from endovascular intervention begins in the prehospital setting.
- Several prehospital stroke scales exist, but have not been validated using arterial imaging to determine the presence of LVOS.
- The Field Assessment Stroke Triage for Emergency Destination (FAST-ED) scale (see Table 1) was designed based on items of the NIH Stroke Scale (NIHSS) with higher predictive value for LVOS.
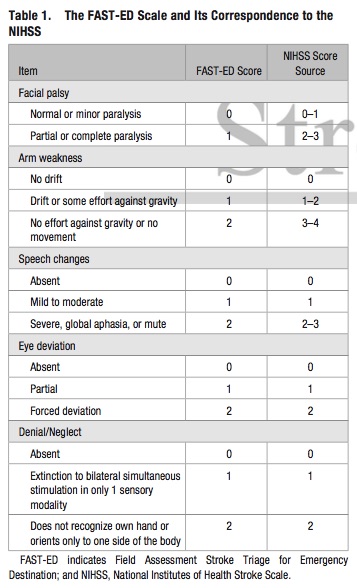
- The FAST-ED scale has comparable accuracy to predict LVOS to the NIHSS, and higher accuracy compared to the Rapid Arterial Occlusion Evaluation (RACE) and the Cincinnati Prehospital Stroke Severity (CPSS) scale
- The FAST-ED scale also provides 3 distinct groups for the likelihood of LVOS:
- Score 0 or 1: <15%
- Score 2 or 3: 30%
- Score >= 4: >60%
Bottom Line: Additional assessment of gaze deviation, aphasia and neglect, as included in the FAST-ED scale, increases the accuracy of predicting LVOS.