Question
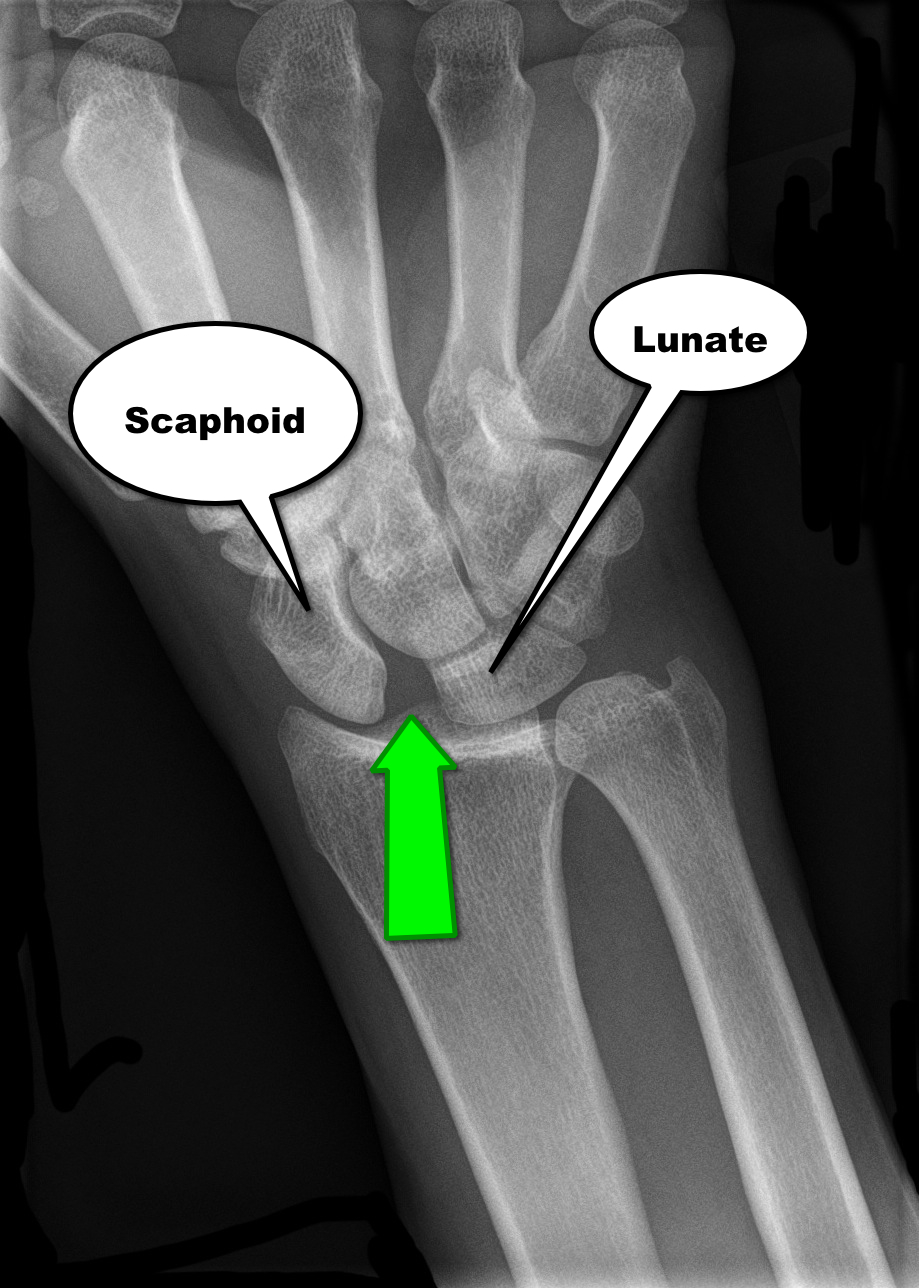
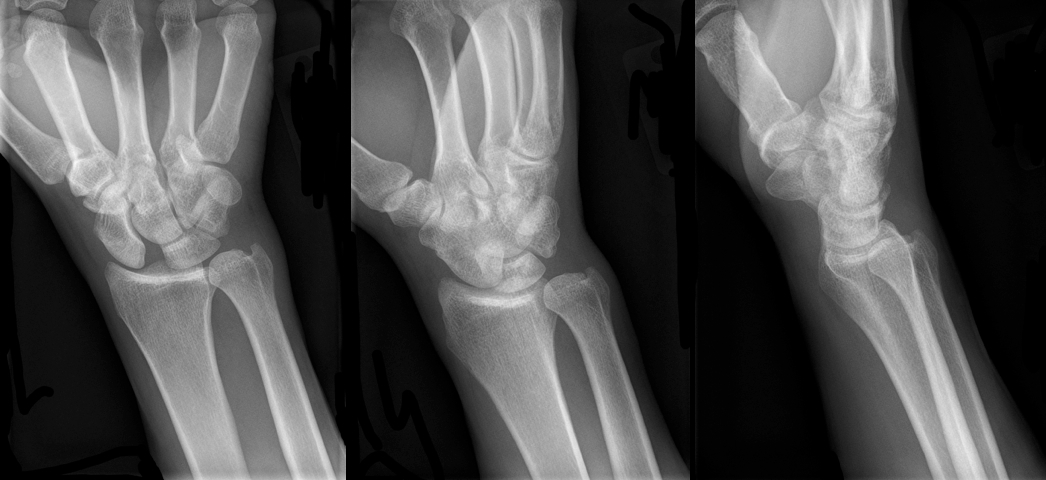
30 year-old male presents with right wrist pain after falling off his bicycle. What's the diagnosis?
Adhesive capsulitis aka frozen shoulder
idiopathic loss of BOTH active and passive motion (this is a significant reduction of at least 50%)
Motion is stiff and painful especially at the extremes
Occurs due to thickening and contracture of the shoulder capsule
Affects patients between the ages of 40 and 60
Diabetes is the most common risk factor
Imaging is normal and only helpful to rule out other entities such as osteophytes, loose bodies etc.
Treatment includes NSAIDs, moist heat and physical therapy.
Patients should expect a recovery period of 1-2 years!
Ultrasound findings of appendicitis
Ultrasound images:
http://www.youtube.com/watch?v=d9jKM6x52nk
http://sonocloud.org/watch_video.php?v=MWHM3D7KD25H
http://sonocloud.org/watch_video.php?v=54862AYWGHGA
Utilizing 20% lipid emulsion at a dose of 1.5 mL/kg (100 mL Bolus) IV with repeat in 15 minutes in no response is being recommended in patients hemodynamic instabiity due to poisoning.
Probably more effective in lipophilic drugs is a current theory for the mechanism of action - the "lipid sink". The idea is that the lipids envelope the drug pulling it off its receptors or sequestering it in the intravascular space. A recent paper has added another mechanism - direct inotropic and lusiptropic effects.(1)
Also, if you think the therapy is experimental, think again. Another recent paper surveyed Poison Control Centers and found 30/45 Poison Centers in the US have a defined protocol for utilization of lipid emulsion therapy. The PCCs are recommending it more.(2)
What was once considered just a purely experimental therapy only used at the very end of code is becoming more mainstream. Comfort with its safety profile and anectodotal effiicacy continues to mount.
Clinical Presentation:
- A 40-year-old Hispanic man was admitted to the hospital after being found unconscious. He had a 2-day history of disorientation that manifested itself as his being unable to recognize family members.
- Upon admission he regained consciousness, becoming alert and oriented, but developed urinary retention and was unable to move or feel his lower extremities.
- Spinal MRI (with and without gadolinium) showed the spinal cord to be abnormally diffuse, with swelling and edema in the cervicothoracic region.
Diagnosis:
- After an extensive work up for lymphoma and CNS infection, he was discovered to have toxoplasmosis and was found to be HIV positive, which was previously undiagnosed.
Discussion:
- Approximately 10% of patients with AIDS present with some neurological deficit as their initial complaint, and up to 80% will have CNS involvement during the course of their disease.
- Myelitis is a known complication of AIDS and is occasionally the initial complaint.
The incidence of myelopathy may be as high as 20%, with 50% of the cases reported post-mortem
- Toxoplasmosis is the most common cause of cerebral mass lesions in patients with AIDS
Occurring in 3–10% of patients in the United States and in up to 50% of AIDS patients in Europe, Latin America, and Africa
Bottom Line:
New neurological deficit in any patient should raise suspicion of HIV infection
Most patients with AIDS that present with evolving myelopathy, characterized by extremity weakness, sensory involvement, spinal cord enlargement, enhancing lesions in brain or spinal cord CT or MRI, have toxoplasmic myelitis
University of Maryland Section of Global Emergency Health
Author: Terrence Mulligan DO, MPH
The Macklin Effect
Pneumomediastinum (click here for image) may be caused by many things:
The "Macklin Effect" is typically a self-limiting condition leading to spontaneous pneumomediastinum and massive subcutaneous emphysema after the following:
Pneumomediastinum secondary to the Macklin effect frequently leads to an extensive workup to search for other causes of mediastinal air. Although, no consensus exists regarding the appropriate workup, the patient's history should guide the workup to avoid unnecessary imaging, needless dietary restriction, unjustified antibiotic administration, and prolonged hospitalization.
Treatment of spontaneous pneumomediastinum includes:
30 year-old male presents with right wrist pain after falling off his bicycle. What's the diagnosis?
Fabella Syndrome
The fabella is a sesamoid bone that is embedded in the tendon of the gastrocnemius muscle where the fibers of the popliteus, arcuate complex and the fibular-fabellar ligament attach.
Fabella syndrome is a painful condition of the posterolateral knee that is exacerbated when the knee is extended. The pain can be exacerbated by palpation of the fabella and if it is compressed against the condyles. The condition is most common in adolescence, but occurs in adults too.
Consider this condition in patients with posterolateral knee pain, which can also be due to tears of the posterior horn of the lateral meniscus, and tendonitis of the lateral head of the gastrocnemius.
General information:
· Salmonella typhi – transmission through fecal-oral, contaminated food, human carriers
· Most cases in the US acquired abroad – Africa, Latin American, Asia
· Vaccine available – not life-long immunity, need 1-2 weeks to take effect
Clinical Presentation:
· sustained high fever (103-104)
· Faget sign: fever and bradycardia (also seen in yellow fever, atypical pneumonia, tularemia, brucellosis, Colorado tick fever))
· Abdominal pain, GI bleed/perforation, hepatosplenomegaly, delirium
· “Rose spots” – erythematous macular rash over chest and abdomen
· Without treatment sx can resolve after 3-4 weeks, mortality from secondary infections 12-30%
Diagnosis:
· Pan-culture for S. typhi
· Serologic: Widal test (negative for 1st week of symptoms, 7-14 days to result)
Treatment:
· Abx: amoxicillin, trimethoprim-sulfamethoxazole, and ciprofloxacin
· MDR typhoid: ceftriaxone or Azithromycine 1st line
Bottom Line:
· Get vaccinated if travelling to endemic areas 1-2 weeks before travel
· Suspect in travelers to endemic areas with sustained high fevers
· Spontaneous resolution does occur but may become carriers without abx
Famous victims or Typhoid fever:
· Wilbur Wright (Wright brothers)
· Prince Albert (Queen Victoria’s husband)
· Hakaru Hashimoto (discovered Hashimoto’s thyroiditis)
· Abigail Adams (1st Lady, wife of John Adams)
University of Maryland Section of Global Emergency Health
Author: Veronica Pei, MD
Monitoring Hyperosmolar Therapy
60 year-old male with a history of pulmonary fibrosis presents to the Emergency Department after a lung biopsy. He is complaining of facial swelling and dyspnea. What's the diagnosis?

Diffuse Idiopathic Skeletal Hyperostosis
aka 1) ankylosing hyperostosis, 2) Vertebral osteophytosis
Large amount of osteophyte formation in the spine, confluent, spanning 3 or more disks
Most commonly seen in the thoracic and thoracolumbar spine.
Osteophytes follow the course of the anterior longitudinal ligaments.
2:1 male to female ratio. Most patients >60yo.
Sx's: Longstanding morning and evening spine stiffness.
PE: Spinal stiffness with flexion and extension.
Dx: plain films
Tx: NSAIDs and physical therapy
http://www.learningradiology.com/caseofweek/caseoftheweekpix2013%20538-/cow542-1arr.jpg
Strychnine poisoning is still occasionally found in rat poisons and in adulterated street drugs and herbal products. The typical symptoms are involuntary, generalized muscular contractions resulting in neck, back, and limb pain. The contractions are easily triggered by trivial stimuli (such as turning on a light) and each episode usually lasts for 30 seconds to 2 minutes, for 12 to 24 hours. Classic signs include opisthotonus, facial trismus, and risus sardonicus.
Differential diagnosis includes:
Case Presentation:
A Spanish speaking man in his late 20s is brought in by ambulance for severe dyspnea. Given the language barrier and his clinical status you are unable to obtain any history. He is tachypnic, had a low pulse ox, and was placed on BiPAP. On exam you hear bibasilar rales and a faint holosystolic murmur.
Clinical Question:
What should be included in the differential?
Answer:
Rheumatic heart disease is the result of valvular damage due to an abnormal immune response following a group A streptococcal infection. It affects 15.6 to 19.6 million people worldwide. Most patients present with dyspnea between the ages 20-50. The most common valvular disease is mitral insufficiency, but it may present with mitral stenosis or aortic regurgitation. The disease is most prevalent in sub-Saharan Africa and among the Indigenous population of Australia but it can be found in many developing countries. People who live in rural areas without access to medical care are those at highest risk for developing rheumatic fever and subsequently rheumatic heart disease.
Bottom Line:
Rheumatic heart disease should be considered in patients who present from an endemic region.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
Fluid boluses are often administered to patients in shock as a first-line intervention to increase cardiac output. Previous literature states, however, that only 50% of patients in shock will respond to a fluid bolus.
Several validated techniques exist to distinguish which patients will respond to a fluid bolus and which will not; one method is the passive leg raise (PLR) maneuver (more on PLR here). A drawback to PLR is that it requires direct measurement of cardiac output, either by invasive hemodynamic monitoring or using advanced bedside ultrasound techniques.
Another technique to quantify changes in cardiac output is through measurement of end-tidal CO2 (ETCO2). The benefits of measuring ETCO2 is that it can be continuously measured and can be performed non-invasively on mechanically ventilated patients.
A 5% or greater increase in end-tidal CO2 (ETCO2) following a PLR maneuver has been found to be a good predictor of fluid responsiveness with reliability similar to invasive measures.
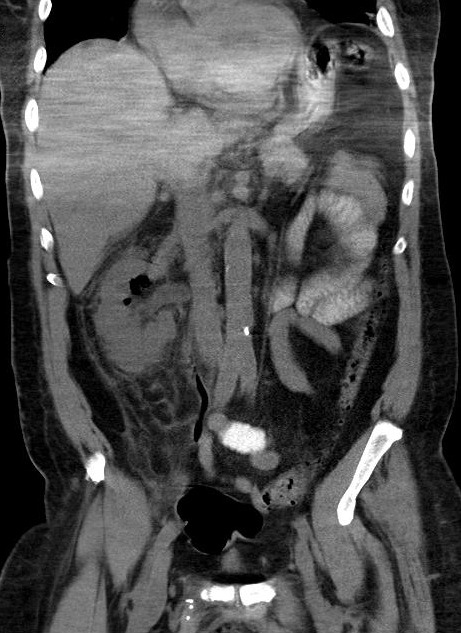
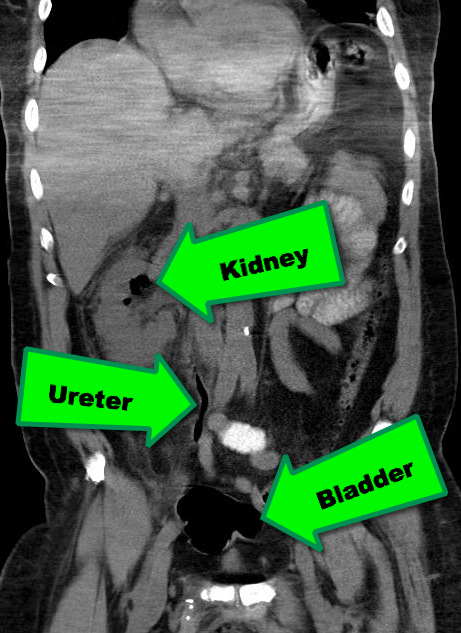
38 year-old male with a past medical history of diabetes presents with back pain and hypotension. CT scan is shown below. What's the diagnosis?