Linezolid is used for gram-positive infections resistant to conventional therapy (e.g., Vancomycin-resistant enterococcus and Methicillin Resistant Staph Aureus). Linezolid is an oxazolidinone, but more importantly it is a weak monoamine oxidase inhibitor (MAOI) and serotonin syndrome (e.g., altered mental status, neuromuscular abnormalities, autonomic instability) may occur when combined with selective serotonin re-uptake inhibitors (SSRIs) or with recent discontinuation of SSRI.
Be aware that the following drugs can precipitate serotonin syndrome when combined with Linezolid:
Mirtazpine Buproprion Fentanyl
Trazodone Buspirone Bromocryptine
Levodopa Lithium Amphetamines
Cocaine Codeine Reserpine
Ergots MAOI's
Got Symptomatic Hypertension? Why not try Fenoldopam?
Fenoldopam is a rapid-acting vasodilator.
Dosing (Adult): After a starting dose of 0.1 to 0.3 mcg/kg/minute, the dose is titrated at 15 minute intervals, depending on the BP response. May be increased in increments of 0.05 to 0.1 mcg/kg/minute every 15 minutes until target blood pressure is reached. Maximal infusion rate reported in clinical studies: 1.6 mcg/kg/minute.
Onset/duration: 5-10 minutes/~ 1 hour.
In order to minimize interruptions in compressions due to pulse checks, continuous end tidal CO2 (ETCO2) monitoring during compressions is recommended. Before spontaneous circulation returns, the ETCO2 is likely to be on the order of < 10 mmg Hg. At the moment spontaneous circulation returns, the ETCO2 is expected to abruptly increase to at least 35-40 mm Hg. Be wary, though, that the administration of sodium bicarbonate may transiently increase the ETCO2 even in the absence of return of spontaneous circulation (ROSC).
Use of ETCO2 in this manner allows one to assess the patient for ROSC without ever having to stop compressions for pulse checks.
Dr. Corwell covered Spondyloysis in July 2010 https://umem.org/res_pearls_referenced.php?p=1134 but if you are like me you might have trouble remembering the differences between the following terms:
We've all been there. It's 2am, and a 4 week old with a temperature of 38.1 rolls in the door. You grab the LP kit and your "best holder." This person then holds the baby's head and neck flexed with one hand, while the other brings the bottom and legs up to the chest as much as possible...all, usually, without pulse oximetry monitoring.
Toxic Holiday Plants
Of the three plants listed, which is NOT poisonous?
1. Holly plant
2. Poinsettia
3. Mistletoe
Poinsettia plants were once thought to be very poisonous. Contrary to popular belief, poinsettias are safe to have in the home during the holidays.
Although there are reported cases of death with ingestion of Holly plants in older literature, recent experience shows gastrointestinal effects in small doses, and serious toxicity such as CNS depression in large ingestions.
Mistletoe ingestion of few of the berries would, at most, produce mild gastroenteritis; however, ingesting concentrated extracts of the plant, including the berries, may produce serious effects such as seizures, mental confusion, drowsiness, and hallucinations.
Happy holidays!
Beware Trendelenburg Positioning in the Critically Ill Obese Patient
In the second half of pregancy, we've traditionally learned that the gravid uterus compresses the inferior vena cava and therefore decreases cardiac output when patient is in a supine position. Therefore, we've learned that patients in the second half of pregnancy the patient should be placed in a left lateral tilt position.
However, it is difficult to perform good quality chest compressions when the patient is in a titled position.
Therefore, the optimal position for chest compressions on the patient in cardiac arrest in the second half of pregnancy is to have the patient in a supine position; and have another rescuer manually deflect the uterus to the patient's left side. This provides optimal compressions + optimal venous return.
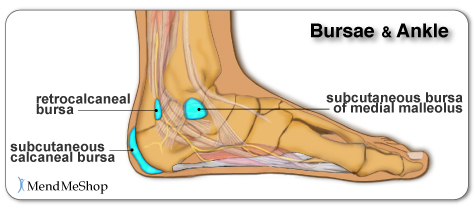
Chief complaint: “Posterior heel pain”
http://www.aidmybursa.com/_img/ankle-retrocalcaneal-subcutaneous-bursitis.jpg
Retrocalcaneal bursitis
The retrocalcaneal bursa is located between the Achilles tendon and the posterior superior border of the calcaneus.
H&P: Inflammation and pain may follow repetitive dorsi/plantar flexion of the ankle (excessive running, jumping activities). Tenderness anterior and superior to the Achilles insertion on the heel.
Treatment: Minimize weight bearing. ½ inch elevation. NSAIDs.
Posterior calcaneal bursitis
This bursa is subcutaneous, just superficial to the insertion of the Achilles tendon.
H&P: Inflammation and pain may follow irritation from the upper border of the heel counter of a shoe. Posterior heel pain. Tender “bump” (the inflamed and swollen bursa) on the back of the heel.
http://podiatry.files.wordpress.com/2006/12/patient2.jpg
Treatment: Opened-heeled shoes, sandals, or placement of a “U-shaped” pad between the heel and the counter. NSAIDs. Advance to shoes with soft or less convex heel counters.
As we eat our turkey today and the myth that we are tired because of the tryptophan content is propagated further - nothing to do with the 2000kcals that we just ate - I would like to share an interesting and controversial study.
Use of stimulants and and sedatives by EM residents. Incidence is as follows:
In a study of 485 residents with 47% response rate:
Prescription Stimulants: 3.1%
Sleep Aids (all): 89%
Use of Nonbenzodiazepines (zolpidem): 14%
Use of Melatonin: 10%
Benzodiazepines: 9%
Difficult job with difficult hours. What is the appropriate medication or is there a medication that truly assists with performance? Are they doing harm to themselves? to patients?
Disrupted circadian rhythm, addiction tendencies and the hardship of a stressful nightshifts are the price we pay for this specialty. Awareness and education are needed for the residents as well as the attendings.
Non-Convulsive Status Epilepticus (NCSE) is generally under reported. An ICU study found 10% admissions for altered mental status (AMS) were eventually diagnosed as NCSE.
Pearls:
- Include NCSE in the AMS differential
- NCSE may occur with or without convulsive seizures
- Difficult to distinguish from a post-ictal state (14% of convulsive seizures convert to
NCSE)
- Reported mortality is up to 44%
Consider NCSE when:
- Seizure history / recent seizures
- Post-ictal period >1 hour
- Odd behaviors (e.g., chewing, blinking, personality change) and abnormal eye
movements (86% specific)
- AMS without structural, metabolic or traumatic etiology
- Patient intubated for status epilepticus
If you are unsure but suspicious of NCSE order a STAT EEG. Treat NCSE like a convulsive status.
We mentioned atropine's elimination from the cardiac arrest (asystole, PEA) protocols last week. Atropine (0.5 mg) is still indicated in unstable bradycardias that appear to be vagally-mediated, such as sinus bradycardia and Mobitz I bradycardia.
Beware, however, that atropine is not recommended in patients with transplanted hearts. These hearts lack vagal innervation, and in fact there's one small study suggesting that atropine may be associated with paradoxical slowing of the heart rate and worsening AV block. Go straight to pacing with these patients.
Evaluation of Potential Intra-Articular Joint Lacerations
Skin and soft tissue injuries in proximity to a joint often prompt concern of whether the injury violated the joint space. Joint Space involvement is important to exclude as it can lead to septic joints and long term disability.
One easy way to determine if the joint capsule has been violated is to inject methylene blue into the joint and watch to see if any of the methylene blue extravasates through the soft tissue.
Indications for a methylene blue injection include:
There are no absolute contraindications. Though clearly the procedure does not need to be done when the injury highly suggests an open joint injury and the patient will require operative debridement and exploration.
To watch a video of a injection head to eMedicine by clicking http://emedicine.medscape.com/article/114453-overview
In the setting of a patient suffering from an anticholinergic overdose with hallucinations/agitation, it may be beneficial to administer the antidote: Physostigmine. Many hesitate simply because they have never administered before or there may be doubt in the diagnosis. Here is the skinny:
1) Anticholinergic OD seen in following meds: diphenhydramine (Benadryl), dimenhydrinate (Dramamine), scopolamine, benztropine (Cogentin), some plants like datura stromonium (thorn apple)
2) Physostigmine 1mg IV slowly over a REAL 5 min. Administer to fast and patient may seize. Maximum dose of 2mg IV.
3) Contraindications: suspicion of TCA OD (anectdotal and from old case report) - screening EKG should be done prior to administration of physostigmine. Also glaucoma, closed angle, obstructive uropathy.
Remember your clinical endpoint needs to be measurable, thus hallucinations and agitation should be reversed. No indication if the patient is only experiencing dry mouth or other more mild anticholinergic symptoms.
-- CSF reforms within 6 hours, making its removal short-term, unless there is a CSF leak.
-- LP can be challenging in obese patients and uncomfortable for patients, in general.
-- LP complications such as low pressure headaches, CSF leak, CSF infection, and intraspinal epidermoid tumors.
Positioning for Ventilated, Critically Ill Obese Patients
Dose of Epinephrine for Patients with Anaphylaxis
Many of us are familiar with 0.3-0.5 mg IM of 1:1,000. Important to give IM and not SC.
In severe cases, consider IV Epinephrine:
{kind=link}
{kind=link}