Question
64 year old male with emphysema and stage 4 lung cancer presents in respiratory distress. What's the diagnosis?

Resistance is expected to be limited, with the exception of VRE, and VSE (vanco resistant or sensitive enterococcus faecalis)
Renally excreted
Common side effects: diarrhea, nausea, headache
Serious side effects: anaphylaxis, renal failure, hepatitis, seizure
Low incidence of C. difficile
Dose : 600 mg IV (over 1 hour) q12 hours X 5-7 days
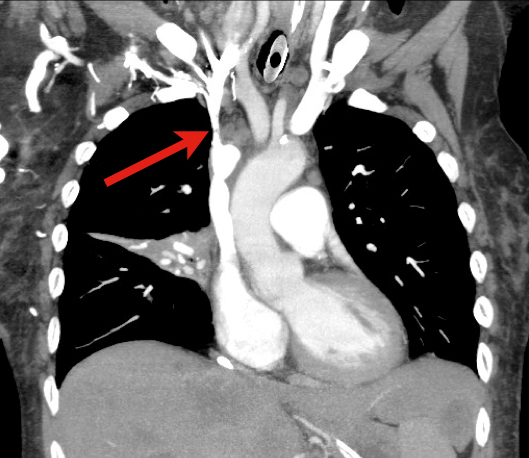
Carotid or vertebral artery injury following blunt trauma is a rare (%1 of blunt trauma), but a potentially serious injury potentially causing stroke and long-term disability.
Injury leads to an intimal tear becoming a nidus for platelet aggregation; thrombosis and/or distal emboli may subsequently develop.
Mechanisms of injury include:
Symptoms of carotid injury may include contralateral sensorimotor deficits; Symptoms of vertebral injury may include ipsilateral facial pain and numbness, headache, ataxia, or dizziness.
Angiography is the diagnostic “gold standard” but these days a 16-slice CT angiography (or greater) is a reliable screening tool.
Anticoagulation with heparin is the treatment of choice for severe injury, if there are no contraindications (e.g., intracranial bleeding). Anti-platelet drugs may be acceptable in certain cases.
Patients with ACS are often treated early with clopidogrel. However, if the patient with ACS appears to be developing cardiogenic shock, its probably best to withhold the early clopidogrel. The literature indicates that patients with cardiogentic shock benefit most from emergent PCI, and many of these patients will need CABG. Generally it's best to avoid clopidogrel in patients heading for CABG.
The use of clopidogrel in patients with cardiogenic shock can be deferred to the cardiologists in the cath lab once they decide whether the patient will need CABG or not.
START Triage
START triage is a simple system to implement that does not require any special equipment in order to determine who needs immediate, delayed or non-urgent care during a mass causality.
START stands for Simple Triage And Rapid Treatment. Patients are triaged based on 4 factors:
The steps are:
So those that can leave are green, those that do not meet any of the START criteria are YELLOW, and those with any of the four factors are RED or DEAD.
Another great example of the generic drug name being so difficult to pronounce you have no choice but to say - Xarelto. The drug touts ease of use and no need for hematologic monitoring like Pradaxa. This drug has the same indication for stroke prevention in nonvalvular atrial fibrillation. It also is being used in DVT prophylaxis in hip and knee surgeries.
Differences:
- Selective Factor Xa inhibitor unlike Pradaxa which is a competetive direct thrombin inhibitor
- Once a day dosing instead of twice a day for Pradaxa
Same concerns:
- No real reversal but can use FFP in a pinch
- Recommend waiting 24 hrs DC med to perform surgical procedure - this includes LP. I am personally waiting for the first case report of LP performed in ED on a patient taking either Xarelto or Pradaxa with subsequent epidural hematoma. Someone is bound to miss this on the med list. Be careful.
Even if your hospital has not added it to its formulary, you will see patients on this drug in the ED.
VBG to Assess Respiratory Function?
64 year old male with emphysema and stage 4 lung cancer presents in respiratory distress. What's the diagnosis?
Feeling a bit guilty about over-eating during these holidays? Here's a study that might make you feel just a tad bit better about those extra pounds. (Just a tad.)
Auer and colleagues reviewed coronary angiograms of over 1000 patients and correlated them with body fat percentage. After statistical analysis, they found that body fat was not associated with the presence (or absence) or severity (size of coronary lesions) of atherosclerosis in men or women. Furthermore, the results did not differ based on age.
What's the takeaway point? Simple: go ahead and have that second serving of ham and eat that extra slice of cake!
[disclaimer: This study has not necessarily been reproduced, and is not intended to give free license to gorge after the holidays are done. It is fully expected that starting on January 2 you will immediately forget all of the above and renew your commitment to a healthy lifestyle consisting of a bland diet and P90X or Insanity workouts on a daily basis. But until then, forget the guilt!]
The long head of the biceps originates from the glenoid tubercle and superior labrum.
Rupture of the proximal biceps tendon comprises 90-97% of all biceps ruptures
Often in men aged 40-60y
- Almost exclusively involves the long head.
- Aka "Popeye Arm" (distal contraction of the muscle belly)
- May be acutely traumatic or microtears & age associated degeneration
- Minimal loss of function because short head of biceps remains attached
- Many patients can be treated non operatively
- Most asymptomatic after 4-6 weeks
- Place in sling, ice, analgesia
- Refer to ortho for re-evaluation and determination of operative versus conservative management
http://imaging.birjournals.org/content/15/4/193/F7.large.jpg
Generally H2O2 is available OTC at a concentration of 3-9% and used as an antiseptic. Toxicity is by two methods: local irritation like a caustic and gas formation - both directly correlating with the % concentration. Some interesting findings have occurred with this ingestion including:
1) Portal vein gas seen on CT
2) Arterialization of O2 resulting in CVA
3) Encephalopathy with cortical visual impairment
4) MRI showing b/l hemispheric CVAs
Even use of 3% H2O2 for wound irrgation has caused subcutaneous emphysema and O2 emboli.
Treatment: XR/CT/MRI may detect gas, if present in RV should be placed in Tredelenburg and carefully aspirated through a central venous catheter. Anectdotal case reports have used HBO therapy when patients were critically ill.(1)
--- Venous drainage obstruction (i.e. cerebral venous sinus thrombosis).
--- Endocrine (i.e. obesity, hypothyroidism, Cushing's disease, Addison's disease).
--- Medications (i.e. vitamin A, cyclosporine, lithium, lupron, oral contraceptives,
amiodorone, and antiobiotics such as tetracyclines and sulfonamides).
--- Other conditions (i.e. pregnancy, steroid withdrawal, acromegaly, polycystic ovary
syndrome, systemic lupus erythematosus, sleep apnea, HIV).
Amiodarone-induced lung toxicity (ALT) is a serious and sometimes fatal complication of amiodarone use.
Symptoms range from mild (e.g., dyspnea with exertion) to acute respiratory distress syndrome and risk of death.
ALT is secondary to either release of toxic oxygen radials that are directly toxic to the lung or the reaction is secondary to an indirect immunologic reaction.
Risk factors for ALT: use > 2 months, dose > 400mg/day, advanced age, or pre-existing lung injury
ALT is typically a diagnosis of exclusion so suspect ALT through a detailed history; physical exam and radiology are non-specific. Lung biopsy is the only confirmatory test.
Treat ALT by discontinuing the drug, steroids, and supportive care. In rare cases where amiodarone cannot be safely discontinued (i.e., life-threatening arrhythmia), dosage should be reduced and steroids added immediately.
Generally, ALT is reversible with a good prognosis.
There are a handful of conditions associated with a rightward axis on the ECG: left posterior fascicular block, ventricular ectopy, lateral MI (old), pulmonary hypertension (acute or chronic), right ventricular hypertrophy, hyperkalemia, misplaced leads, and toxicity of sodium channel blocking drugs, to name a few.
When you notice that the rightward axis is NEW compared to an old ECG, and there's nothing else on the ECG that's obviously diagnostic (e.g. hyperkalemia would also show peaked Ts; ventricular tachycardia would be wide complex and fast, etc.), in emergency medicine you should always think first and foremost of the following three possibilities:
1. acute pulmonary embolus
2. toxicity of a sodium channel blocking drug
3. misplaced leads
Pay attention to axis! Using the above rule can make rightward axis very simple and useful.
AM
Pediatric forearm fractures:
The Crashing Patient with PAH
Metaphyseal bucket handle and corner fractures are almost pathognomonic for child abuse
These injuries were originally identified by clinicians evaluating children with subdural hematomas
These injuries are typically seen in the ankles, knees, elbows and wrists
Violent twisting, shaking, or pulling across a joint creates shearing forces across the weak epiphyseal growth plate and metaphysis
This leads to
1) A thin rim of mineralized metaphyseal bone aka “bucket handle”
http://rad.usuhs.mil/rad/home/peds/bucketarrow.jpg
OR
2) Small flecks of bone from the metaphyseal corner adherent to periosteum
http://t2.gstatic.com/images?q=tbn:ANd9GcT0kZ3VR1f7MwRj7oIa6jaYVp_-f8kZ1NhSbw4kCTRGNLDJ1pKK9g