NSSTIs occur secondary to toxin-secreting bacteria; NSSTIs are surgical emergencies with a high-morbidity / mortality
Risk factors: immunocompromised host (DM, AIDS, etc.), intravenous drug use, malnourishment, peripheral vascular disease
Type I (polymicrobial; most common), Type II (monomicrobial; typically clostridia, streptococci, staph, or bacteroides), Type III (Vibrio vulnificus; seawater exposure)
Signs / Symptoms: pain out of proportion to exam (occasionally no pain at all), skin findings (blistering / bullae, gray-skin discoloration, or “Dishwater-like” discharge), or systemic toxicity (altered mental status, elevated lactate, etc.)
Diagnostic radiology
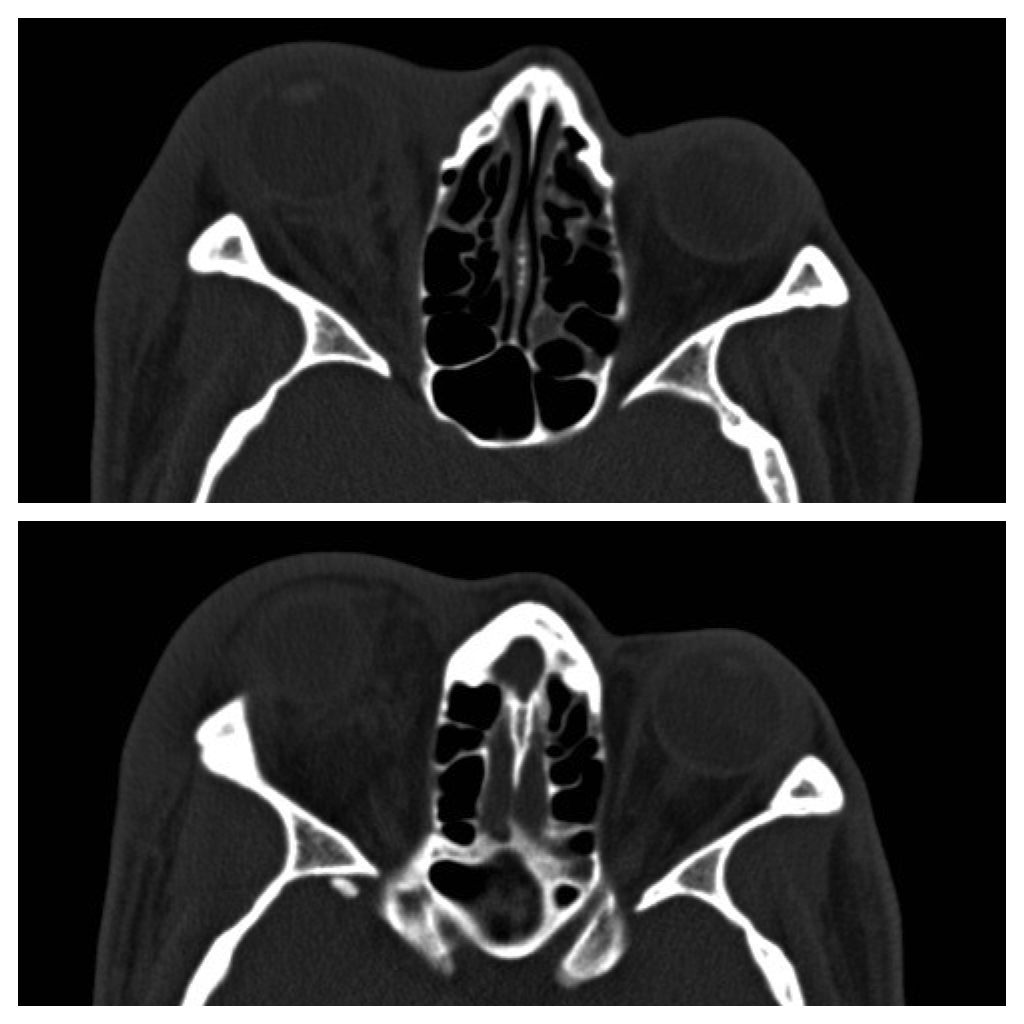
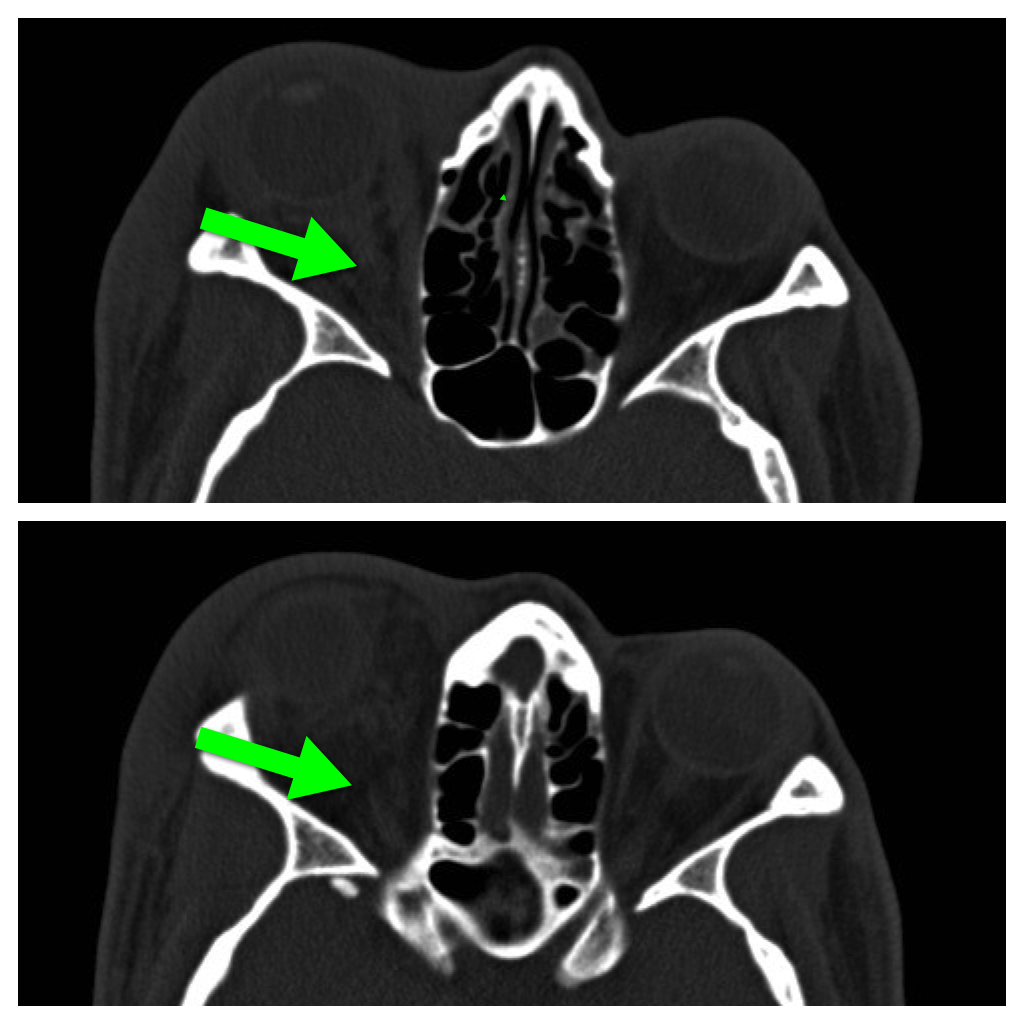
- Xray (shows gas); low sensitivity; CT scan (gas / tissue stranding); sensitivity is also low
- MRI can over-diagnose NSSTI and should not be used routinely
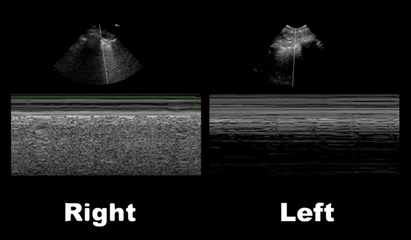
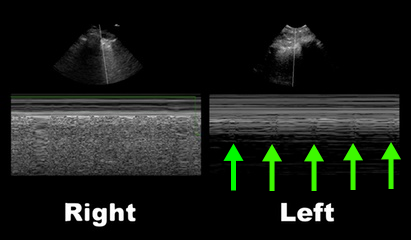
- Bedside ultrasound may demonstrate fluid or gas collections in deeper tissues (see clip below)
Treatment is emergent surgical debridement with simultaneous hemodynamic resuscitation PLUS broad-spectrum antibiotics; consider clindamycin becuase it has anti-toxin activity
Adjunctive therapies include Intravenous intraglobulin (neutralizes toxins secreted by bacteria) and hyperbaric oxygen