Question
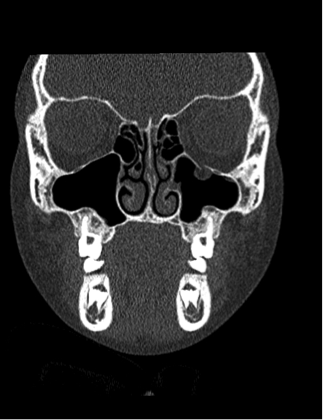
8 year-old female presents with nausea, vomiting, double-vision and inability to move her left eye upwards after being kicked in the face at school. What's the diagnosis?
There is more than the standard preparations of plasma, platelets, and PRBCs in the blood bank. Certain patients will require these specialized preparations when a transfusion is required. Here are three to know:
8 year-old female presents with nausea, vomiting, double-vision and inability to move her left eye upwards after being kicked in the face at school. What's the diagnosis?
Our suspicion of significant abdominal injury increases when there is bruising across the abdomen in adults after a motor vehicle collision, but what about in children? A PECRAN analysis may have provided us with the answer.
Of 3740 pediatric patients after motor vehicle collision, 16% had a seat belt sign. Seat belt sign was defined as a continuous area of erythema, ecchymosis or abrasion across the abdomen due to the seat belt. 1864 children had CT scans of the abdomen. Intra-abdominal injuries (IAI) were more common in those children with seat belt sign than those without (19% versus 12%). Those with seat belt sign had a greater risk of hallow viscous or mesenteric injuries. There was no increased risk of solid organ injury. 33% of patients with seat belt sign did not have complaints of abdominal pain or tenderness on initial exam (with a GCS of 14 or 15); 2% of these patients underwent operative intervention for their injuries.
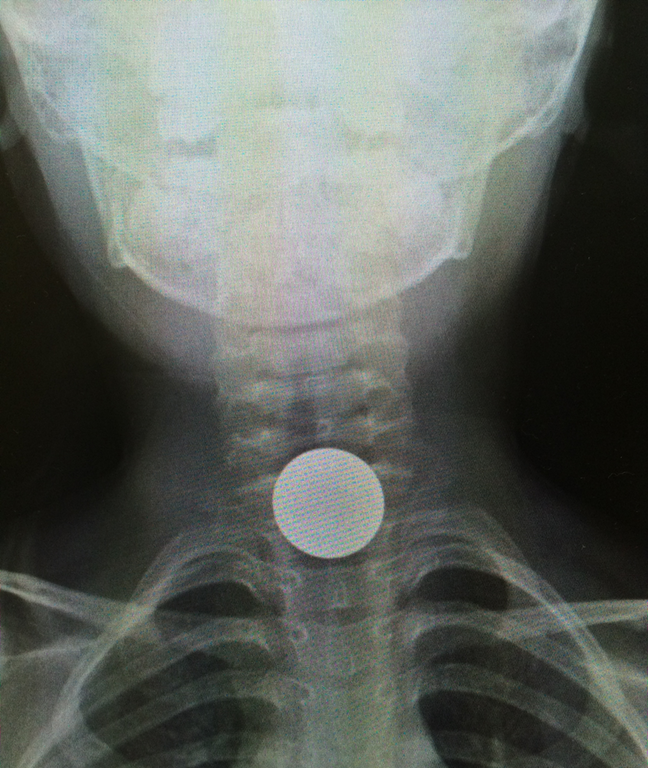
Toxicity due to body packing and body stuffing can be a significant concern due to unknown quantity and/or substance that was ingested.
A recent prospective observational case series compared the utility of CT abdomen/pelvis with and without PO contrast in identifying the ingested packets.
The gold standard comparison: surgical removal or expulsion of packets.
All patients received CT abd/pelvis with and without PO contrast.
A. Body stuffers (n = 24)
CT w/ PO contrast:
Positive: 7 (sensitivity 29.2%)
Negative: 17
CT w/o PO contrast:
Positive: 9 (sensitivity 36.5%)
Negative: 15
All 24 patients passed ingested packets
B. Body packers (n= 11)
CT w/ PO contrast
CT w/p PO contrast
10 patients expulsed packets; one patient did not have any packets.
Conclusion
Bottom line:
Last month we discussed symptoms of serotonin syndrome and its diagnosis by the Hunter Criteria. Let's move on to what causes serotonin syndrome.
Serotonin Syndrome - What Causes It?

** Stay tuned for the conclusion on management of serotonin syndrome **
5 year-old boy who presents with sudden onset hoarse voice, and drooling without a fever.
In patients receiving renal replacement therapy as a treatment modality for dabigatran-related bleeding, watch for a rebound concentration increase after hemodialysis is stopped.
More than 50% of patients demonstrate a rebound effect with a median increase in dabigatran concentration of 33%.
It is unclear whether this rebound effect is clinically important, and whether it translates to prolonged clinically relevant bleeding. Extended hemodialysis sessions or consideration of CVVHD should offset this potential problem.
Bonus Pearl:
The North American Congress of Clinical Toxicology starts today and runs through October 12. Look for toxicology pearls and updates on Twitter under the official conference hashtag #NACCT15.
Overall, suicide is the 15th leading global cause of death. However, it is the 2nd leading cause among 15-29 year olds
Suicides are preventable. Interventions to decrease suicides include:
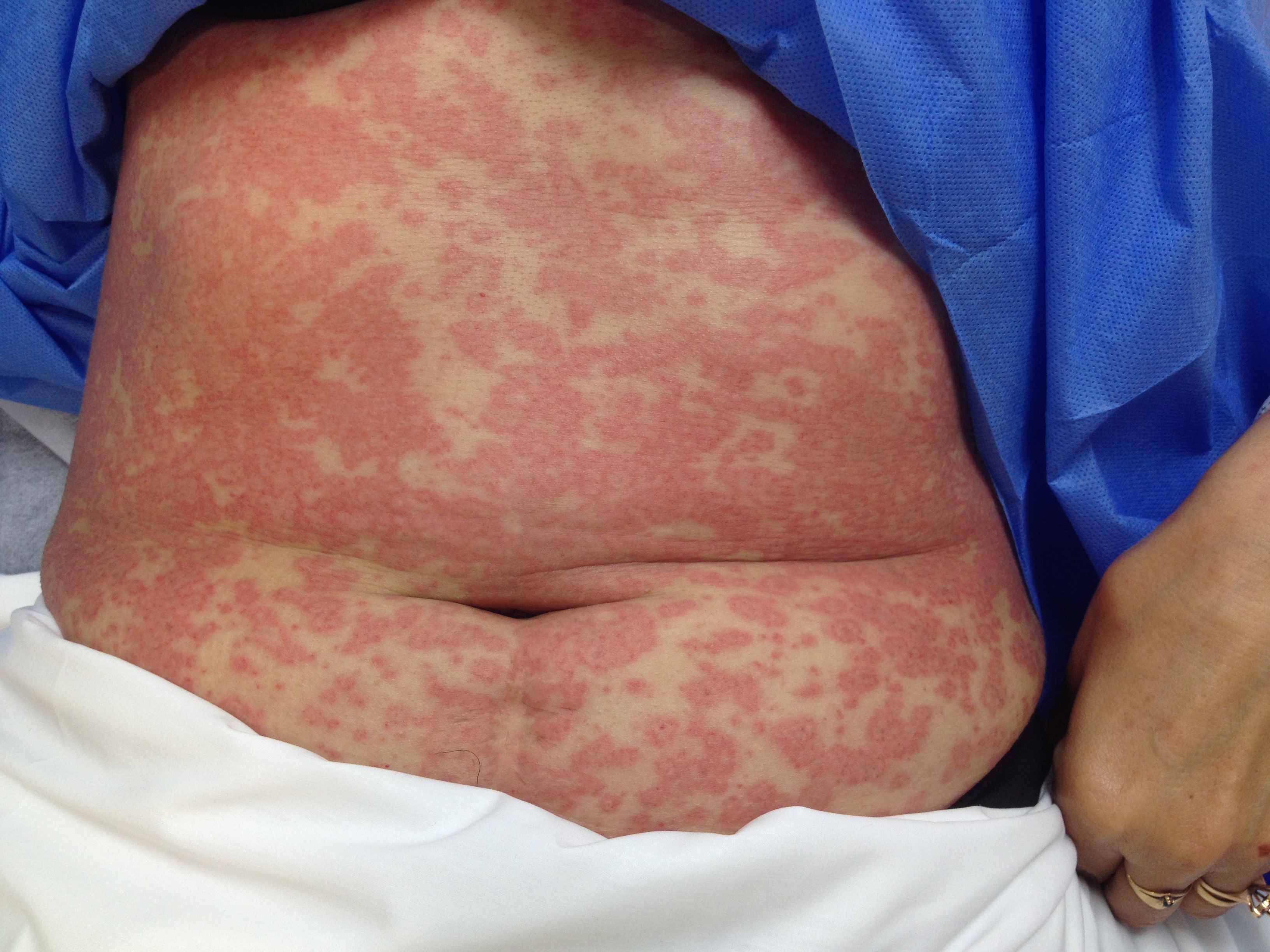
Patient presents after being started on an antibiotic for cellutlitis of lower extremity. What's the diagnosis and what are some other etiologic agents (name 3)
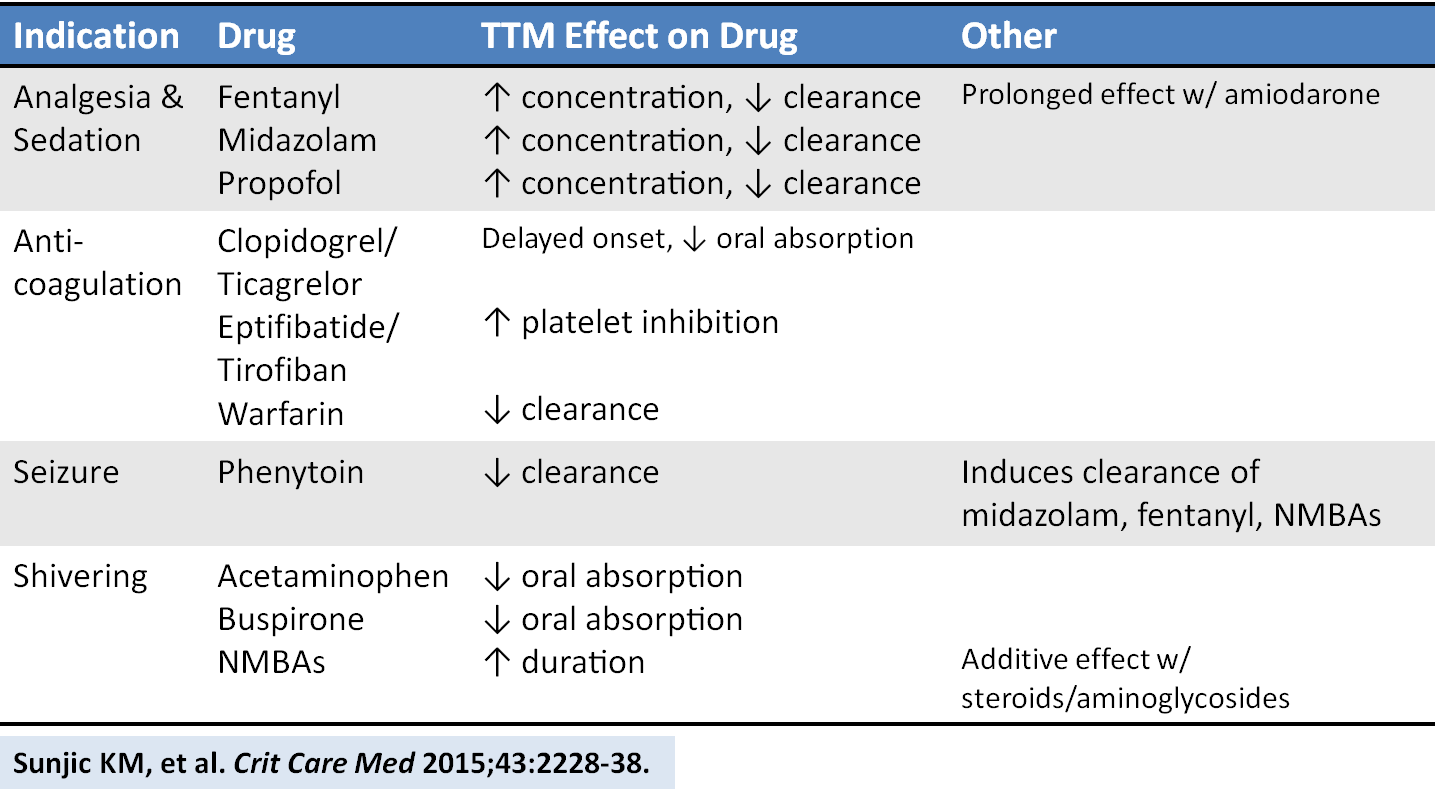
An excellent new review article provides a detailed look at how the drugs we give are affected by targeted temperature management. Here is a helpful chart of drug alterations that have data in reduced body temperature states:
A group from Colorado identified the high-stress of pediatric resuscitation as a high-risk setting for possible medication error. As such, they performed a prospective, block-randomized, crossover study with two mixed teams of docs (ABEM certified) and nurses, managing 2 simulated peds arrest scenarios using either:
1) conventional “draw-up and push” drug administration methods [control] or
2) prefilled medication syringes labeled with color-coded volumes correlating to the weight-based Broselow Tape dosing [intervention].
The objective was to compare the time of preparation and administration of a medication, as well as to assess dosing errors. Participants were blinded to the purpose during recruitment but unblinded just prior to running the scenarios.
The scenarios included advanced airway management and hemodynamic life support efforts to care for an 8-year-old or 8-month-old manikin. The intervention group received a standard 3-minute tutorial on the use of prefilled color-coded syringes just prior to their scenario. After completing the first scenario, the groups switched, utilizing the other sim with the other method of medication administration. After a 4-16 week “wash out” period, the groups reconvened to reverse the medication administration technique across the same 2 scenarios.
Each Broselow tape color zone corresponds to a narrow range of weights. The authors opted to designate medication dosing errors >10% above or below the correct range as critical dosing errors.
The results? Median time to delivery of all conventionally administered medication doses was 47 seconds versus the prefilled color-coded administration system-- 19 seconds. The conventional administration system saw 17% of doses with critical errors versus none for the prefilled color-coded syringe group.
These prefilled color-coded syringes are not currently manufactured. Should they go into commercial production, the hope is that such syringes would be longer and more narrow than conventional syringes to effectively elongate each color-coded section (the delineations for red and purple on a standard syringe differ by as little as 1/8-3/32 of an inch if you want to make your own!-- see picture).
If you are interested in learning about the current status of emergency medicine in a specific country, it can be difficult to find up-to-date information. One excellent resource for country specific details is the American College of Emergency Physicians’ (ACEP) International Ambassador Program.
This program has Emergency Medicine Ambassadors (U.S. emergency physicians), Liaisons (in-country emergency physicians) and Representatives (U.S. emergency physicians in training) for many countries around the world. Additionally, there are country specific reports that give annually updated information about emergency medicine in each country.
Included on the website are links to send emails to the Ambassadors, Liaisons and Representatives in order to request more detailed information.
To learn more, see: http://www.acep.org/IntlAmbassador/
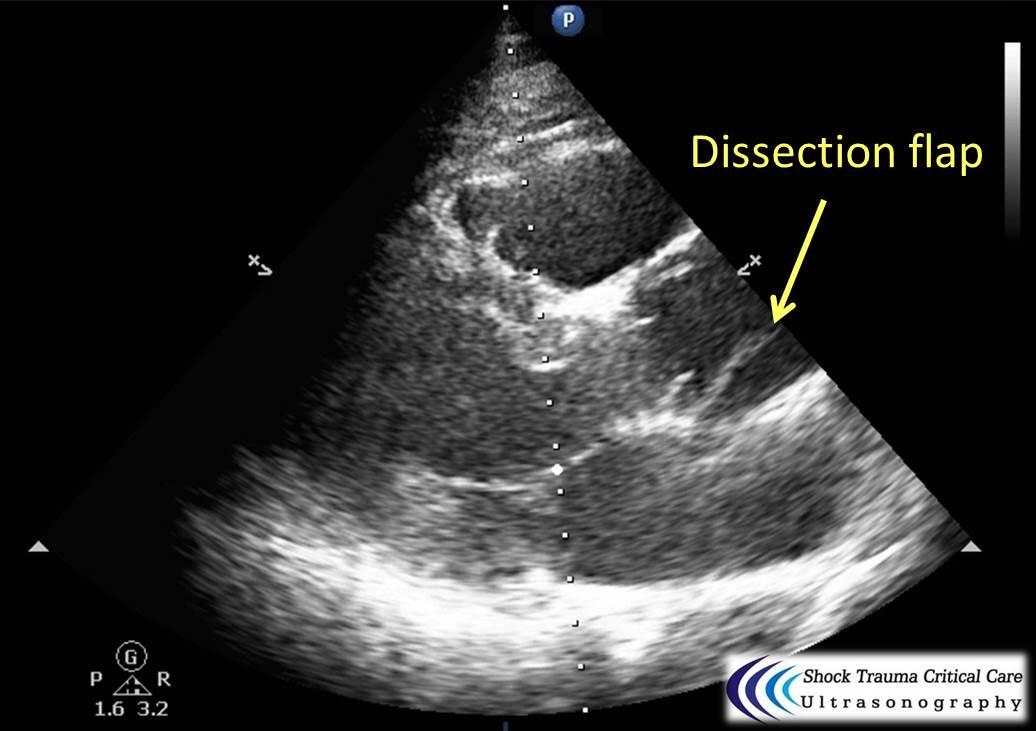
Classically, aortic dissection presents as tearing or ripping chest pain that radiates to the back in a HYPERtensive patient.
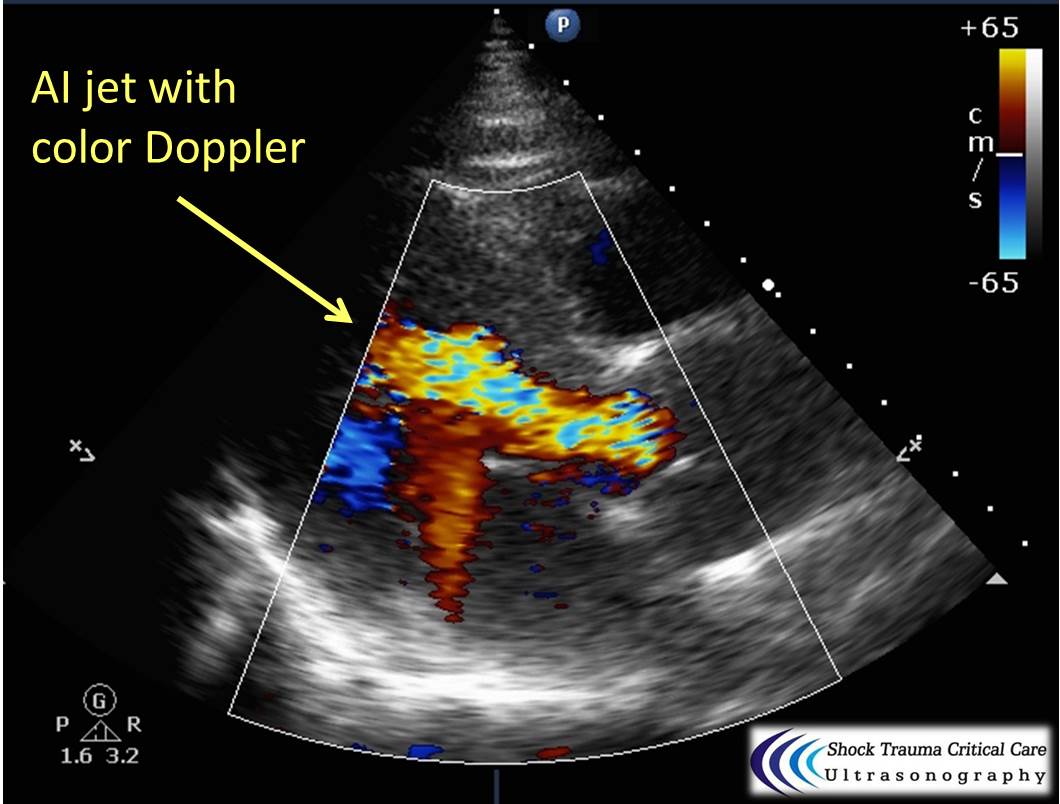
However, type A aortic dissections can quickly become HYPOtensive due to any the primary cardiac complications from retrograde dissection into:
Bedside echo can't rule out aortic dissection, but it can help rule in the diagnosis (figure 1) or complications (figure 2) at times.
26 year-old male presents with a swollen 4th digit and pain during extension, what’s the diagnosis?

Most common mass in popliteal fossa
Incidence 10 to 58%
Intra-articular pathology results in flow of synovial fluid from the joint into the bursa, forming a cyst
Association with concomitant intra-articular disorders 94%
Possible pathology - Meniscus, ligamentous, arthritis, other osteochondral defects
In children this is not a pathologic finding
Symptoms - Posterior knee bulging, posterior tightness/stiffness esp. with knee flexion
Ultrasound - 100% sensitive/specific
DDx: DVT
Tx: Refer for ultrasound guided aspiration, fenestration and steroid injection
http://www.caringmedical.com/wp-content/uploads/2013/11/Bakers-Cyst-treatment.jpg
A thunderclap headache is defined as a very severe headache that reaches its maximum intensity within 1 minute.
One of the most common causes (and the one associated with this buzzword on board questions!) is subarachnoid hemorrhage, but what else can cause a it?
- Reversible cerebral vasoconstriction syndrome (RCVS): suggested by recurrent thunderclap headaches (2-10) over 1 to 2 weeks. Normal CT and LP, with vasoconstriction on angiography. Can lead to SAH, ICH or ischemic stroke.
- Cervical artery dissection
- Cerebral venous sinus thrombosis
- Spontaneous intracranial hypotension: characterized by orthostatic HAs and auditory muffling.
- Intracerebral hemorrhage
- “Primary”: a diagnosis of exclusion
Bottom line? All patients with thunderclap HA should have a stat head CT with no contrast, then have SAH excluded with an LP, CTA or MRI/MRA. Just because you excluded SAH in a patient with thunderclap headache does not mean you’re done with the emergency workup.

30 year-old male with abdominal pain and diffuse tenderness on exam. Ultrasound is shown, what's the diagnosis?