Question
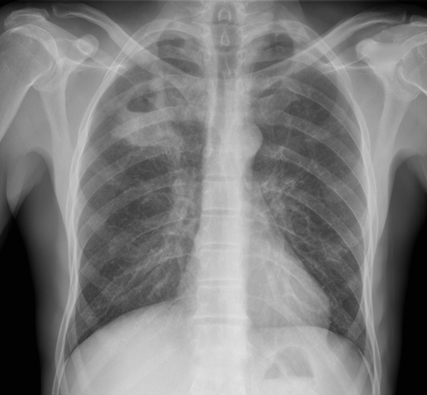
16 yo M with pleuritic right upper chest pain that started today. He is suffering from an asthma exacerbation currently in the setting of URI with cough. He is afebrile, tachycardic to 140-150s, respiratory rate 20, and sats 98% on room air. ECG was performed which incidentally diagnosed this patient WPW and he went for ablation as an outpatient. His chest x-ray showed:
Besides a bad day, what do we call this chest x-ray finding?
Macklin Phenomenon
-asthma exacerbation rupture of the alveoli causing pneumomediastinum
-typically a young man
-most common chief complaint is chest pain
Physical Exam: Hamman’s sign may be present (crackle with heartbeat) or subcutaneous emphysema
Etiology: Esophagus, lungs, or bronchial tree
Rupture of alveoli: asthma exacerbation (bronchial hyper-reactivity/constriction), barotrauma, valsalva maneuvers (lifting, childbirth), deep respiratory maneuvers/Valsalva (strenuous exercise or FVC breathing), drug use (crack cocaine causing bronchial constriction, marijuana), vomiting, blunt thoracic/abdominal trauma, scuba diving with rapid ascent
Aerodigestive tract injuries: bronchoscopy tracheobronchial injuries, laryngeal fx, bronchial fx, tracheal neoplasm, esophageal injuries (Boerhaave syndrome, paripartum, asthma exacerbation, esophageal neoplasm)
Extension from neck: head/neck sx, RPA/PTA, dental abscess/extractions
Extension from RP/chest wall: rupture RP hollow viscus
Management:
-self -limited
-treat underlying condition
-swallow study for all cases following emesis to rule out Boerhaave’s syndrome
-no repeat CXR, advance diet as tolerated, 23 hour observation
-Al-Mufarrei, et al suggest without trauma, pleural effusion, hemodynamic instability, pneumoperitoneum, or severe vomiting, the finding of spontaneous pneumomediastinum (with or without Meckler’s triad of esophageal rupture: vomiting, lower chest pain, and cervical subcutaneous emphysema after overindulgence) usually leads to unnecessary radiologic investigations, dietary restriction, and antibiotic administration
-surgery for decompression
Gray JM and Hanson GC. Mediastinal emphysema: aetiology, diagnosis, and treatment. Thorax. 1966; 21: 325-332.
Al-Mufarrej F, Badar J, Gharagozloo F, Tempesta B, Strother E, Margolis M. Spontaneous pneumomediastinum: diagnostic and therapeutic intervnetions. Journal of Cardiothoracic Surgery. November 2008; 3: 59.
Attachments