What Do You Mean By Dizzy?
- Patients with dizziness account for 3% of ED visits.
- The traditional approach based on symptom quality (i.e. “What do you mean by dizzy”) is not reliable.
- Drs. Edlow and Newman-Toker propose a new paradigm based on the timing and triggers of dizziness.
- Acute vestibular syndrome begins abruptly or rapidly and continues for days. Patients’ dizziness may be exacerbated by movement but is not triggered by movement.
- Triggered episodic vestibular syndrome are repetitive episodes of dizziness triggered by some event. Patients will be completed asymptomatic at rest and will develop dizziness that is reliably triggered by a specific event or postural shift.
- Spontaneous episodic vestibular syndrome are multiple episodes of dizziness that occur without any clear identifiable trigger. Patients are asymptomatic between episodes.
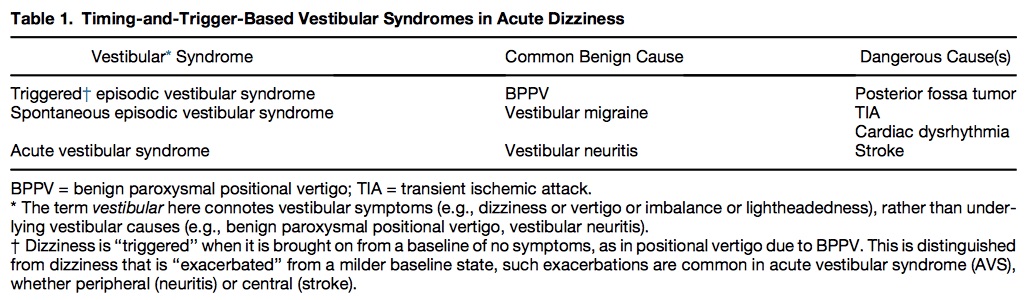
Table 1 shows common benign and serious causes of these vestibular syndromes.
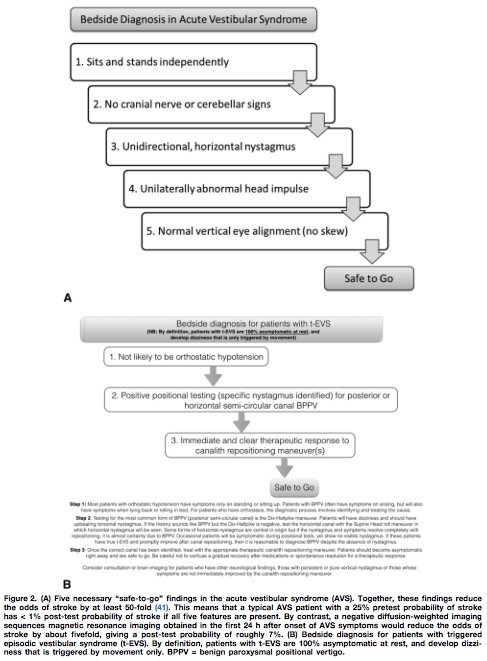
Utilizing the HINTS battery or the Dix-Hallpike maneuver, a “safe to go” algorithm for acute vestibular syndrome and triggered episodic vestibular syndrome is outlined in Figure 2.