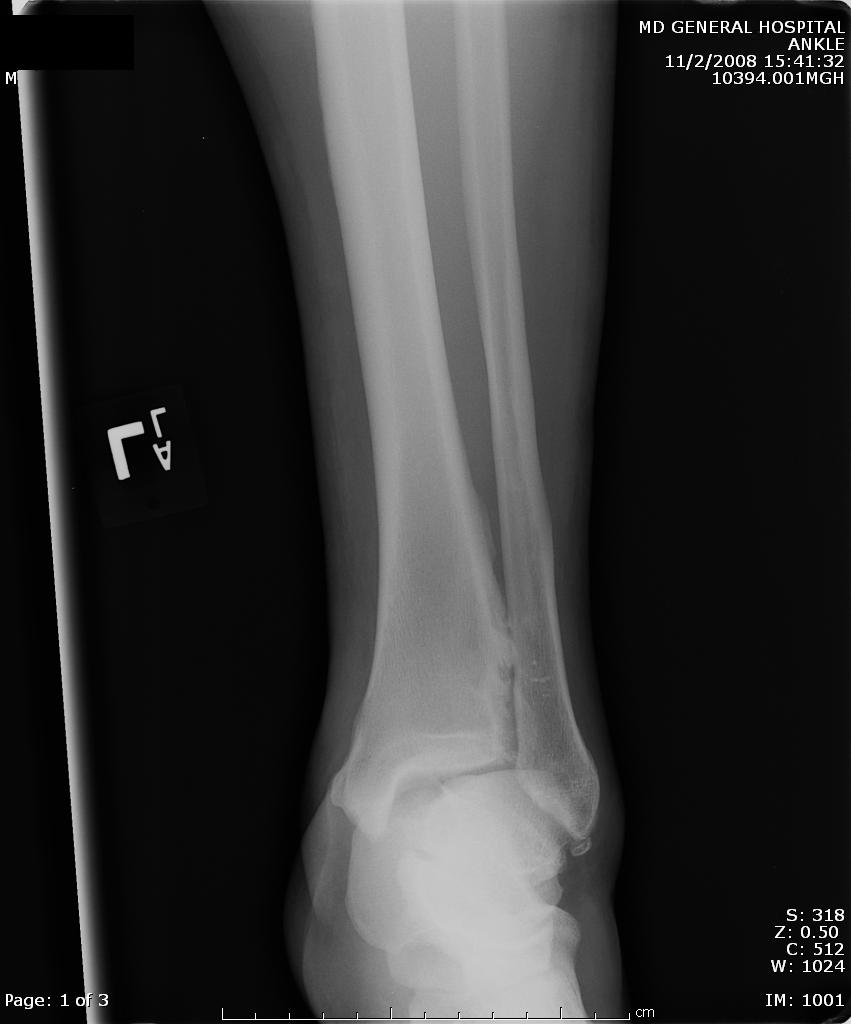
A maisonneuve fracture is a fracture dislocation resulting from external rotational forces to ankle -- through interosseous ligament to fibula.
- Proximal fibula fracture - from external rotational forces (spiral/oblique)
- Ankle components can include any of the following:
- medial maleolus avulsion fx or deltoid ligament rupture
- anterior talofibular ligament rupture
- interosseous ligament rupture
- posterior malleolar fracture
If stability is questionable, orthopedic evaluation under anesthesia is required. Additionally always consider compartment syndrome. Do not rely on Kanduval's signs (pain, paraesthesia, pallor, poikilothermia, pulselessness) - "... with the exception of pain and paraesthesia, these traditional signs are not reliable." Emergent orthopedic consultation and compartment pressure assessment should be performed. (see attached photos)




{kind=link}
{kind=link}
{kind=link}