Classically, aortic dissection presents as tearing or ripping chest pain that radiates to the back in a HYPERtensive patient.
However, type A aortic dissections can quickly become HYPOtensive due to any the primary cardiac complications from retrograde dissection into:
- The pericardium causing cardiac tamponade
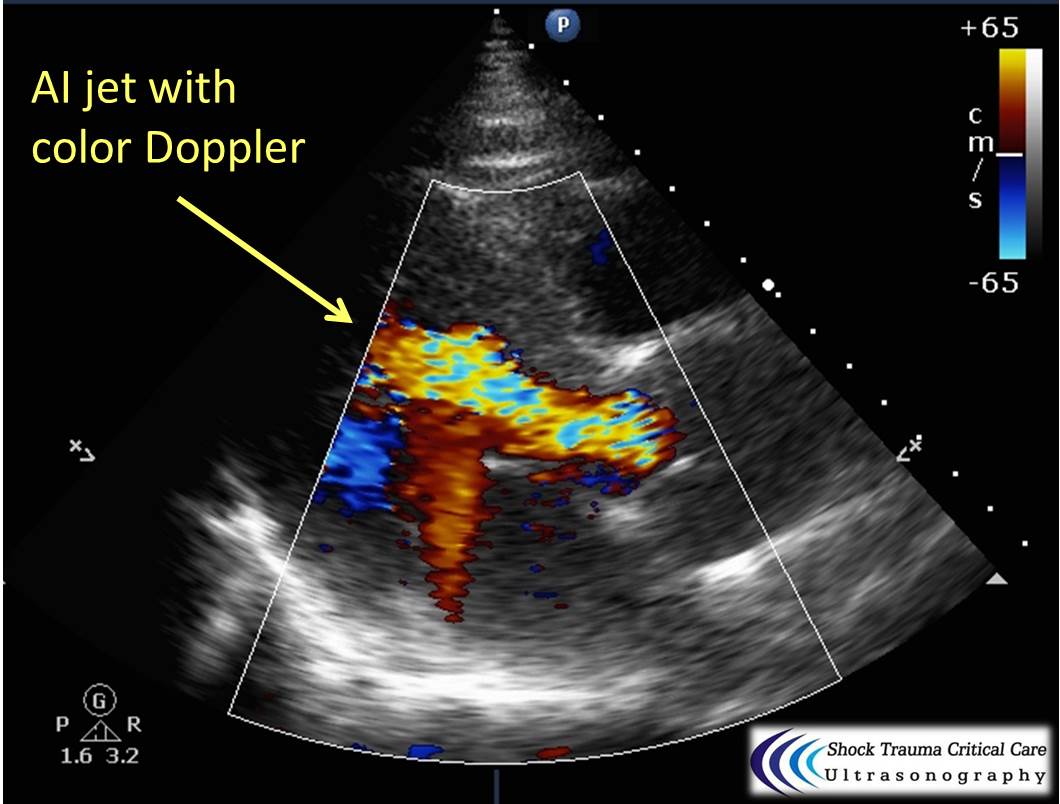
- The aortic valve causing wide-open aortic insufficiency
- One of the coronary arteries (typically the RCA presenting as inferior STEMI)
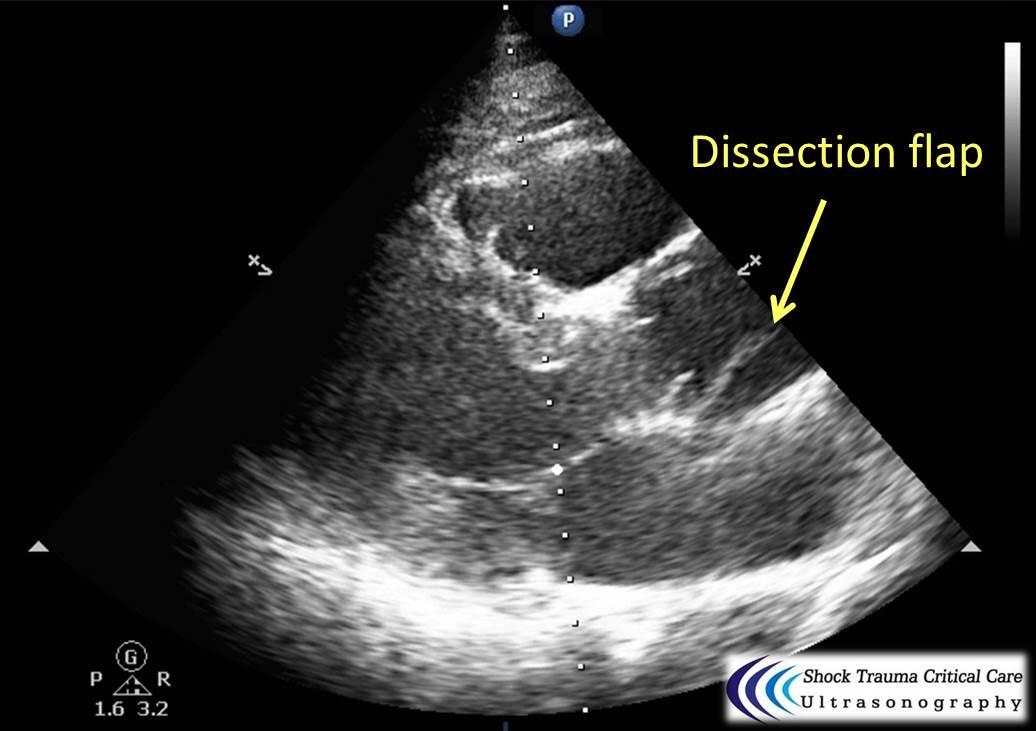
Bedside echo can't rule out aortic dissection, but it can help rule in the diagnosis (figure 1) or complications (figure 2) at times.

{kind=link}