- Intracerebral hemorrhage (ICH) volume is a predictor of mortality and clinical outcome.
- Communicating ICH volume to neurosurgical and neurocritical care consultants can help direct treatment decisions.
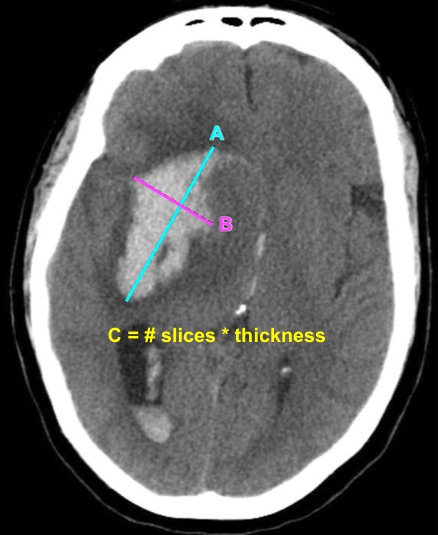
- ICH volume can be estimated using the ABC/2 formula:
- Select the CT slice with the largest area of the hemorrhage (reference slice)
- A = Measure the largest diameter
- B = Measure the largest diameter perpendicular to A
- C = Multiply the number of CT slices with the hemorrhage by the slice thickness
- Slices with 25-75% of the hematoma volume compared to the reference slice count as 1/2 slice
- Slices with <25% of the hematoma volume compared to the reference slice do not count
- A recent study by Dsouza et al. found that EM attendings as well as EM trainees were reliable in estimating ICH volume using ABC/2 compared to radiologists.
Bottom Line: EPs can reliably estimate ICH volume using the ABC/2 formula. Communicating ICH volume to neurosurgical and neurocritical care consultants can help direct treatment decisions.