- We've talked about the rising incidence of cerebral venous thrombosis (CVT) and choice of neuroimaging studies before, now let’s talk about presentation and treatment.
- Symptoms range from headache to coma with cerebral edema and intracranial hypertension depending on the veins and sinuses involved.
- Superior sagittal sinus is most frequently affected (62%) and can cause headache, hemiparesis, hemisensory loss, hemianopia, and seizures.
- Transverse sinus is also commonly involved (45%) and can cause headache, aphasia, and seizures.
- Thrombosis of the deep veins is seen in 18% of cases and can cause altered mental status, coma, and gaze palsy.
- Management includes anticoagulation, treatment of underlying cause, seizures, and intracranial hypertension.
- LMWH is preferred unless in patients with renal dysfunction or need for rapid reversal of anticoagulation.
- Endovascular intervention may be considered in severe cases that do not improve or deteriorate despite anticoagulation.
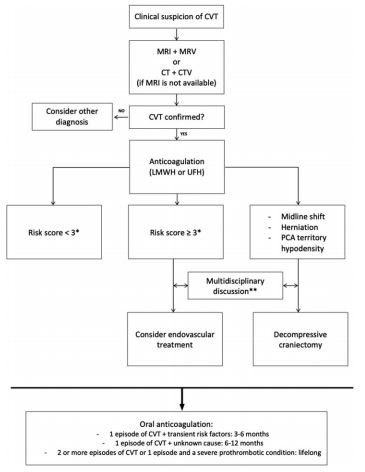
- Poor prognostic factors are:
- 2 points each - malignancy, coma, deep venous thrombosis
- 1 point each - mental status disturbances, male, intracranial hemorrhage
- Score ≥3 suggests high risk of poor outcome
Bottom Line: Severity of CVT presentation depends on the location and clot burden. Anticoagulation is key, though consider endovascular intervention if patient does not improve or deteriorates despite anticoagulation.