Patient-ventilator dyssynchrony is a sign of a disagreement between the patient's breathing and the ventilator's settings. Recognizing and fixing it is a critical skill to prevent lung injury and improve comfort. Ineffective triggering and double-trigger are two common types of dyssynchrony.
Ineffective Triggering
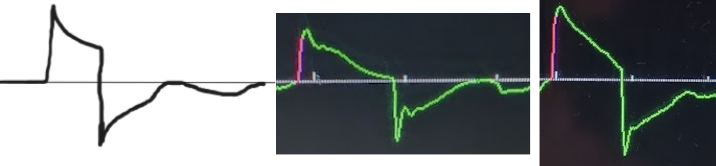
The patient tries to take a breath, but they are too weak to trigger the ventilator. This is the most common type of dyssynchrony. It causes increased work of breathing and discomfort.
Look for a small dip in the pressure waveform and a simultaneous scoop out of the expiratory flow waveform that is not followed by a delivered breath.
Troubleshooting options:
- Try making the trigger more sensitive (e.g., decrease flow trigger from 3 L/min to 1 L/min).
- Try increasing the respiratory support based on the mode of ventilation. The patient may need higher pressure or volume to support the breaths they are able to trigger.
- Check for and treat auto-PEEP, which makes it harder for the patient to trigger the next breath. This is especially critical for patients with COPD or asthma!
- Try a different mode of ventilation
Double-Triggering ("Breath Stacking")
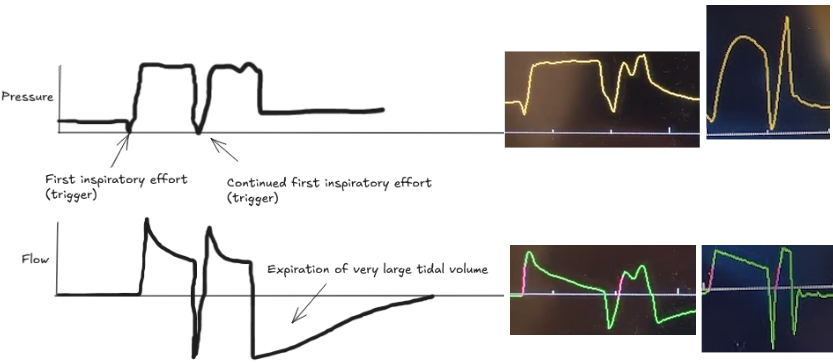
The patient's own breath outlasts the ventilator's set inspiratory time (Ti), causing one patient effort to trigger two stacked breaths. This results in delivery of large tidal volumes, risking lung injury (volutrauma).
Look for two consecutive breaths on the ventilator screen without a full exhalation in between.
Troubleshooting options:
- Increase the set tidal volume Vt or the inspiratory time Ti to better match patient demand.
- Address underlying causes of high respiratory drive (e.g., pain, anxiety, acidosis).
- Increase sedation if appropriate.
- Try a different mode of ventilation, such as pressure support, where the patient has more control over inspiratory time.
Bottom Line
Dyssynchrony means the ventilator settings do not match the patient's needs. Watch the waveforms to diagnose the mismatch, then either adjust the ventilator or treat the underlying problem.