Acute respiratory distress syndrome (ARDS) is an acute, inflammatory lung injury that effects the lung diffusely and can be triggered by various insults. Aside from the Kigali modification, the most recent updated definition of ARDS was the Berlin definition in 2012. There have been many advances and changes in the understanding and clinical practice for managing patients with ARDS since then. In 2024, Matthay, et al. proposed the new global definition to build upon the Berlin criteria [1]. They addressed several important issues with the Berlin definition to improve the diagnostic criteria and improve ability for diagnosis in resource-limited settings.
ARDS Berlin Definition
- Acute onset of respiratory failure or worsening respiratory failure that occurs within one week of a risk factor/insult
- Pulmonary edema is NOT solely due to cardiogenic pulmonary edema or fluid overload.
- Hypoxemia is NOT solely due to atelectasis
- Bilateral opacities on chest imaging (x-ray or CT) that isn’t due to pleural effusion, atelectasis or masses
- PaO2:FiO2 of </= 300 mm Hg with categories of mild (>200 and </=300 mm Hg), moderate (>100 and </= 200 mm Hg) and severe ( </=100 mm Hg) with PEEP or CPAP of 5 cm H20
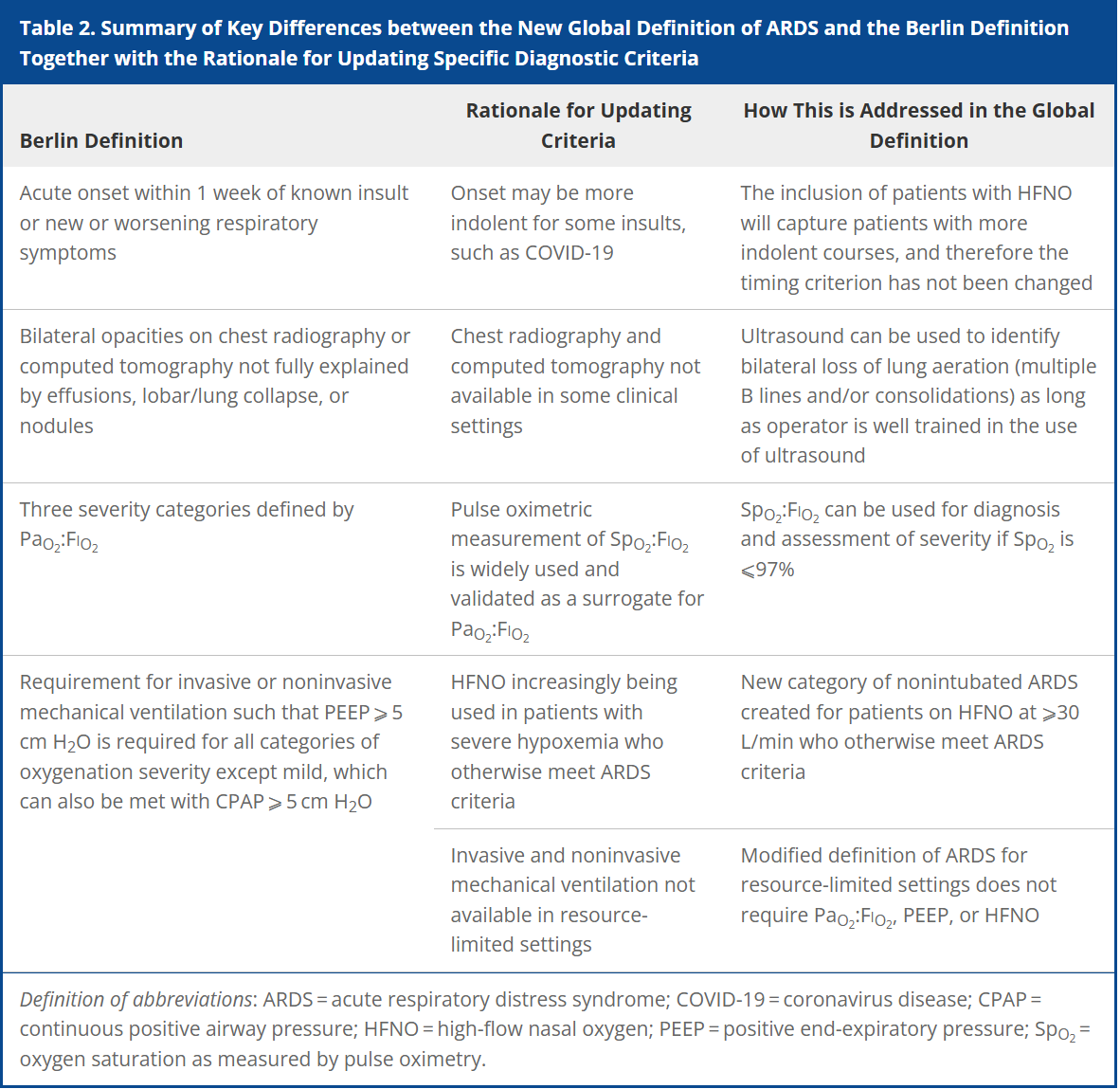
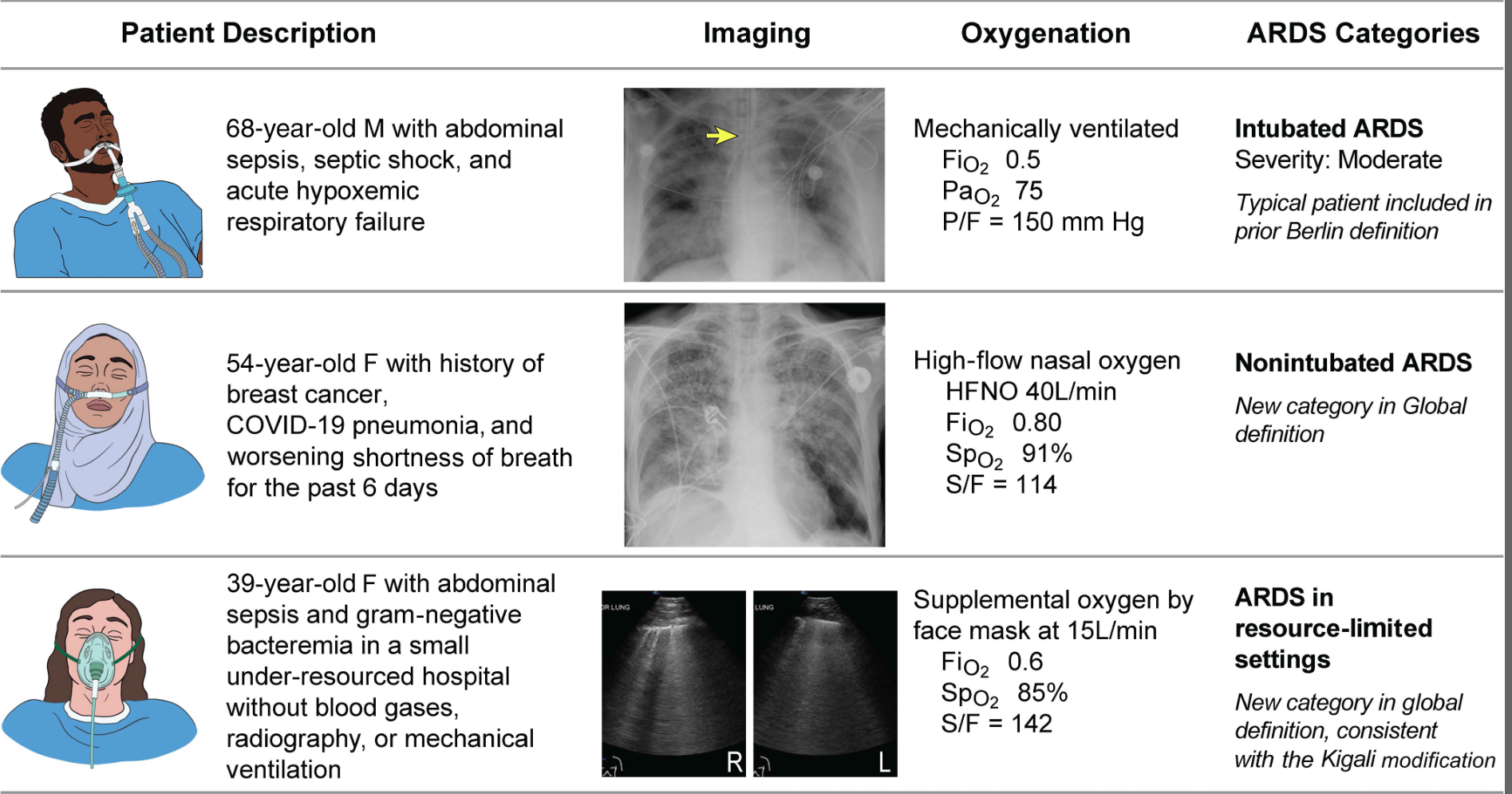
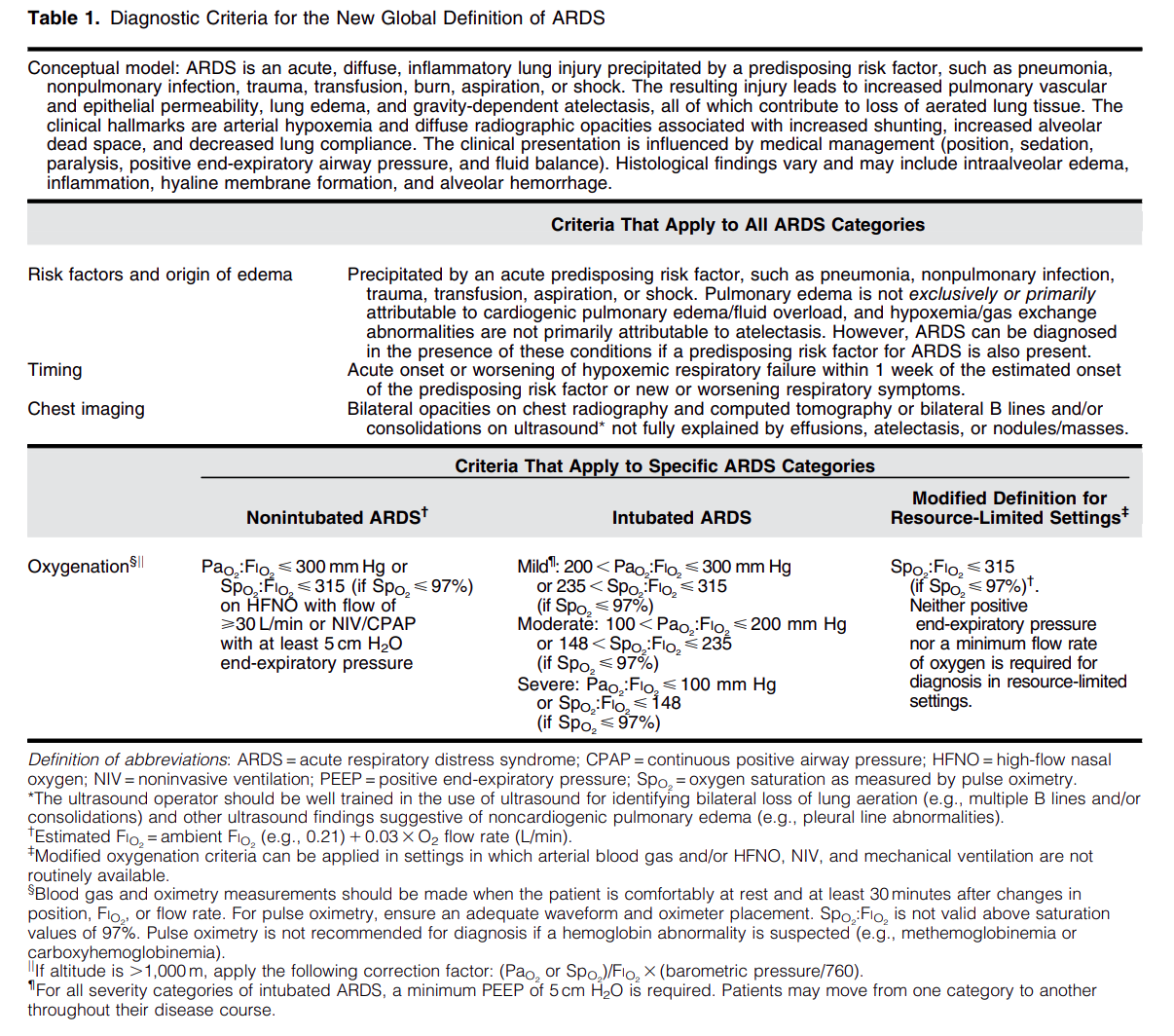
Important updates for the Global definition of ARDS
- Ultrasound can be utilized to diagnose bilateral infiltrates
- SpO2:FiO2 can be used to diagnose and assess severity. SpO2 should be < 97%
- Modified ARDS definition to not require PaO2:FiO2 cutoff (can use S:F ratio instead) or PEEP requirement
- Non-intubated patients who otherwise meet criteria for ARDS and are managed with high-flow nasal cannula (HFNC) with at least 30 L/min of flow would meet the diagnostic criteria
Diagnostic Criteria for the New Global Definition of ARDS from Matthay et al.
The Global Definition of ARDS expands upon the Berlin definition. It was shown that this new definition improves diagnosis in resource-limited settings, allows for earlier detection, and better classification [2]. A retrospective study evaluating this new global definition found that there was a significant number of patients identified using this new definition who would have been missed using the Berlin definition [3]. These patients may benefit from ARDS directed therapies and further prospective studies will be needed to assess how this new definition effects clinical management of these patients using the new definition.