- Neurogenic bladder refers to urinary tract dysfunction associated with neurological conditions.
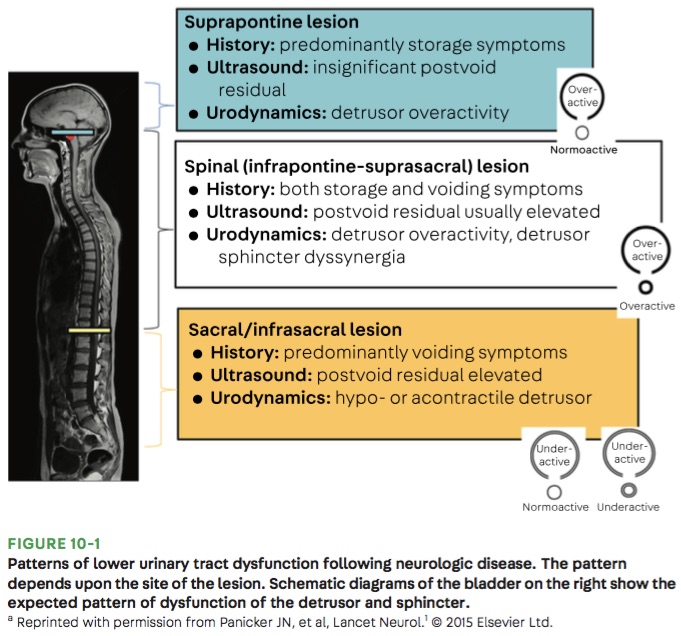
- There are 3 patterns that can occur depending on the location of the neurological injury (see figure below):
- Suprapontine lesions (e.g. Parkinson disease) cause involuntary bladder contractions, resulting in urinary incontinence.
- Infrapontine to suprasacral lesions (e.g. cervical and thoracic spinal cord injuries) cause uncoordinated bladder and urethral sphincter contractions, resulting in incomplete emptying of the bladder and urinary retention.
- Sacral/infrasacral lesions (e.g. cauda equina syndrome) cause poor bladder contraction and/or nonrelaxing urethral sphincter, resulting in urinary retention.
- Medications such as opiates, anticholinergics, and alpha-adrenoceptor agonists can also cause urinary retention.
Bottom Line: Urinary retention can be seen with neurological injury involving the lower brainstem, spinal cord, cauda equina, and peripheral nerves.