By performing a Point-of-Care Transvaginal Ultrasound (TVUS), we can decrease length of stay for patients with early pregnancy. Moreover, if an ectopic pregnancy is identified, we can decrease time to the OR for these patients.
Begin by discussing the exam with the patient and ensuring they have emptied their bladder. Apply a probe cover and add sterile lubricant to the outside of the probe tip. You can save time by performing a TVUS immediately after the pelvic speculum exam for swab collection.
- Obtain a Sagittal View of the Uterus:
Gently introduce the transducer with the marker upward, directed towards the ceiling. As you slowly advance, the uterus will be visualized in a sagittal orientation. Fan through the uterus by moving the probe handle left and right.
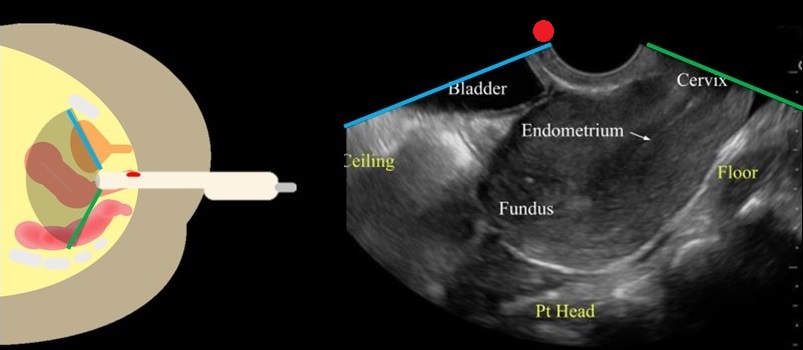
Image From: doi: 10.1016/j.emc.2022.12.006.
- Obtain a Coronal View of the Uterus:
Rotate the transducer so that the marker is directed towards the patient's right side. Fan through the uterus by lifting the probe handle up and down.
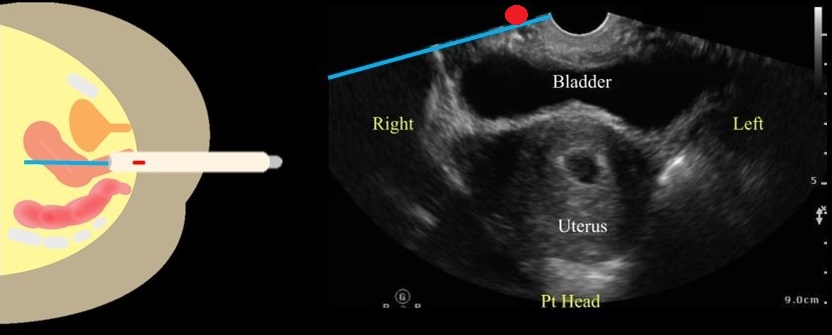
Image From: doi: 10.1016/j.emc.2022.12.006.
If a gestational sac is found, you should measure the gestational age and if present, fetal heart rate.
Tilt the transducer towards the patient's left or right side to visualize the adnexa. The adnexa will be located medially to the iliac vessels.
Remove the transducer and follow your department protocol for high level disinfection.
Salerno A, Lewiss RE. Rekindling the Relevance of Obstetrical Transvaginal POCUS: Overcoming Barriers to Ensure Patient-Centered Care. POCUS J. 2023 Nov 27;8(2):106-108. doi: 10.24908/pocus.v8i2.16855. PMID: 38099157; PMCID: PMC10721291.
King SA, Salerno A, Sommerkamp S. Ultrasound in Pregnancy. Emerg Med Clin North Am. 2023 May;41(2):337-353. doi: 10.1016/j.emc.2022.12.006. Epub 2023 Feb 9. PMID: 37024168.