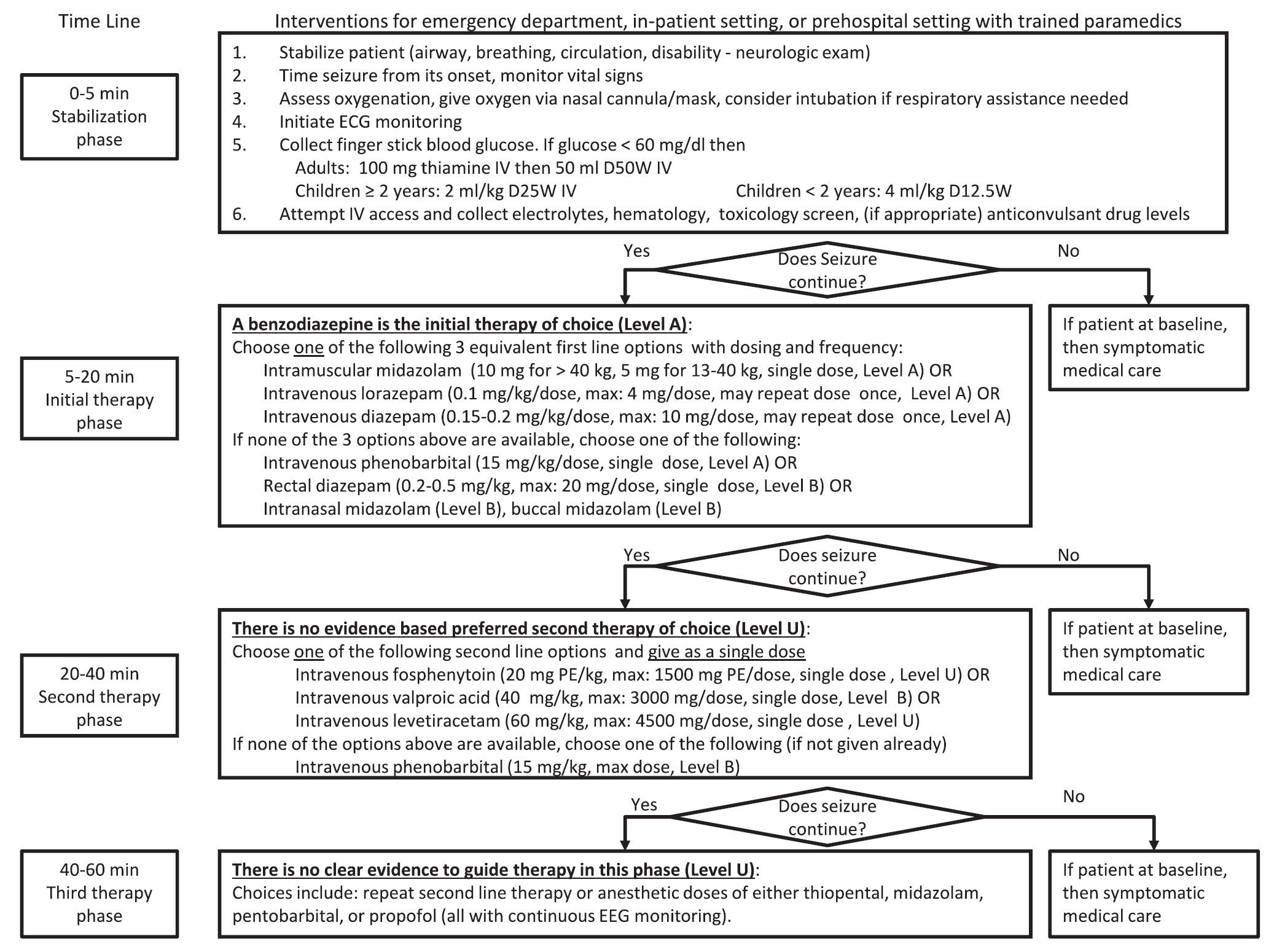
A new guideline for convulsive status epilepticus in adults AND children was recently published. [1] An insightful commentary was published alongside it (both are open access). [2] The proposed algorithm is below. Here are a few additional points to note:
- The guideline applies to convulsive status epilepticus.
- A new level of evidence rating of "U" is utilized. It means "data inadequate or insufficient; give current knowledge, treatment is unproven."
- It addresses 5 specific questions:
- Which anticonvulsants are efficacious as initial and subsequent therapy?
- What adverse events are associated with anticonvulsant therapy?
- Which is the most effective benzodiazepine?
- Is IV fosphenytoin more effective than IV phenytoin?
- When does anticonvulsant efficacy drop significantly?
- IM midazolam is incorporated as one of the recommended 1st choices of treatment.
- One of the second phase therapy recommendations is levetiracetam 60 mg/kg! It is a level U recommendation. Be prepared for neurology to request this dose. There is no data in adults to support this high of a dose.