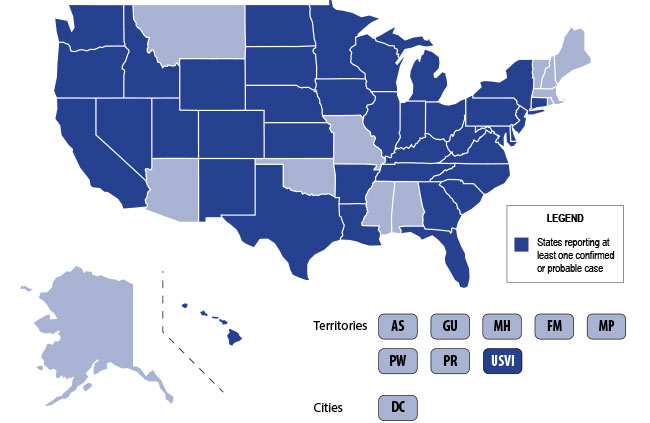
The U.S. is currently experiencing an epidemic of a severe lung disease termed Vaping-Associated Pulmonary Illness (VAPI), with over 500 cases and 7 deaths across 38 states and 1 U.S. territory since July 2019.
The clinical presentation of VAPI varies --
- Respiratory (SOB, cough, chest pain), constitutional (fever, tachycardia, headache, dizziness), and potentially GI symptoms (vomiting, diarrhea) after the use of vaping devices. GI symptoms may precede respiratory issues.
- Can take days or worsen over weeks and can present or end up with severe respiratory failure
Diagnostics --
- Labs nonspecific: Leukocytosis, elevated ESR, no specific infectious etiology
- Chest CT generally with bilateral infiltrates
- Bronchoscopy with BAL demonstrates PMNs and may have lipid-laden macrophages on Oil red O or Sudan staining
Treatment is supportive +/- steroids --
- Current recommendations to treat similarly to ARDS in intubated patients
- Potential benefit to steroids if not contraindicated
Bottom Line: Include vaping-associated pulmonary illness in your differential for patients presenting with acute lung disease.
- Ask patients about use of e-cigarette/vaping devices.
- Notify the CDC or your state health department of any suspected cases.
- Counsel your patients to avoid the use of these devices, at the very least until the specific causative agent is found.