While the invasive monitoring of central venous pressure (CVP) in the critically ill septic patient has gone the way of also transfusing them to a hemoglobin of 10 mg/dL, it remains that an elevated CVP is associated with higher mortality1,2 and renal failure.2,3
Extrapolating from existing data looking at hepatic vein, portal vein, and renal vein pulsatility as measures of systemic venous hypertension and congestion,4,5,6 Beaubien-Souligny et al. developed the venous excess ultrasound (VExUS) grading system incorporating assessment of all 3, plus the IVC, using US to stage severity of venous congestion in post-cardiac surgery patients.7 They evaluated several variations, determining that the VExUS-C grading system was most predictive of subsequent renal dysfunction.
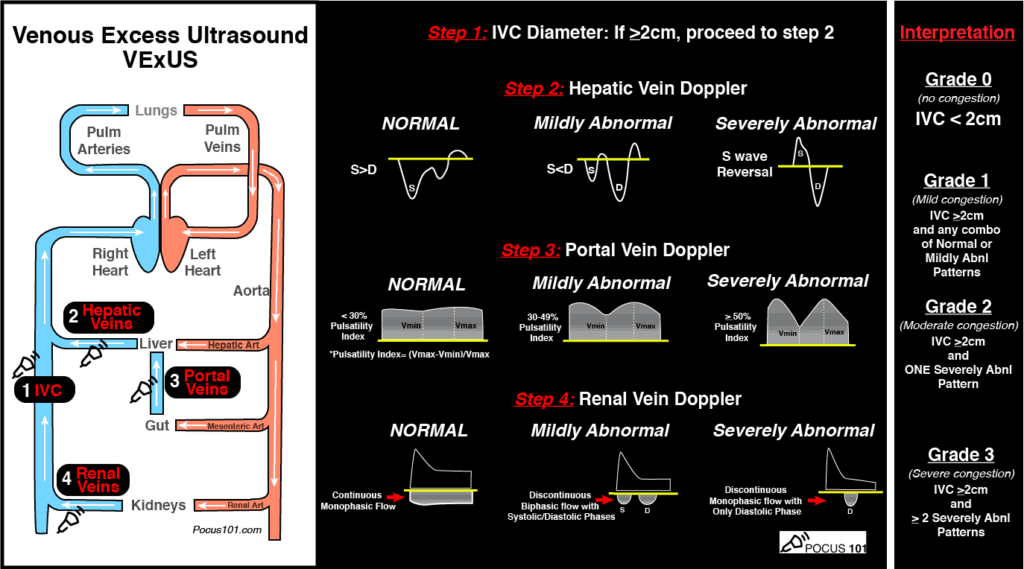
(Image from www.pocus101.com)
High Points
VExUS Grade 3 (severe) venous congestion:
- Correlated with higher CVP & NTproBNP levels, as well as overall fluid balance
- Had a 96% specificity for development of subsequent AKI
Caveats
- Evaluating all parameters yields the most benefit to avoid false positives
- Can be difficult to obtain all views (>25% of subjects excluded due to poor US image quality)
- Studied in a limited population, notably not primarily RV failure patients
Clinical Uses
- To limit harmful fluid administration in shock
- To help answer the prerenal vs cardiorenal AKI question in CHF
- To indicate when volume removal (diuresis) should be the strategy, even in patients with vasopressor-dependent shock
A great how-to can be found here:
https://www.pocus101.com/vexus-ultrasound-score-fluid-overload-and-venous-congestion-assessment/