Question
A patient presents with the rash shown below and is treated with penicillin. Fever, headache, and myalgia develop four hours later. What’s the diagnosis?

A patient presents with the rash shown below and is treated with penicillin. Fever, headache, and myalgia develop four hours later. What’s the diagnosis?
Prior literature has demonstrated the safety and feasibility of placing subclavian lines with ultrasound guidance; here's a link to a short educational video describing the technique.
The literature has been varied, however, as to which approach is best for venous cannulation with ultrasound; the supraclavicular (SC) or infraclavicular (IC) approach (see references below)
A recent study evaluated both approaches in healthy volunteers in order to determine which approach is superior for cannulation using ultrasound.
98 patients were prospective evaluated by Emergency Medicine physicians with training in ultrasound. In each patient, both SC and IC views were evaluated on both the left and right sides; each view was given a grade for ease of favorability (no patients were actually cannulated)
Overall, it was found that the SC view was significantly more favorable compared to the IC view; the right SC was non-significantly preferred compared to the left SC.
The clip below demonstrates normal right femoral anatomy. The structure with the asterisk is the right common femoral vein and the arrow is pointing to a branch of the right femoral vein. What is the name of the branch and what is its importance during lower extremity ultrasound?
66 year-old female presents with one week of epigastric and right flank pain. Urinalysis was normal. What’s the diagnosis?

Only 50% of hemodynamically unstable patients will improve their hemodynamics in response to a fluid bolus. However, because excessive fluid administration can lead to organ edema and dysfunction, it is important to give hemodynamically unstable patients only the necessary amount of fluids to improve their hemodynamics.
There are two general categories of assessing a patient's response to volume administration; static and dynamic assessments (see referenced article below):
Static assessment (generally unreliable, but traditionally used):
Physical exam (dry mucus membranes, cool extremities, etc.)
Urine output
Blood pressure
Central venous pressure via central-line
Dynamic assessment (more reliable but more labor intensive)
Pulse Pressure Variation
IVC Distensibility Index
End-expiratory occlusion test
Passive Leg-Raise
There is no simple way to accurately determine the need for a fluid bolus however the integration of the techniques above can help the clinician make better decisions.
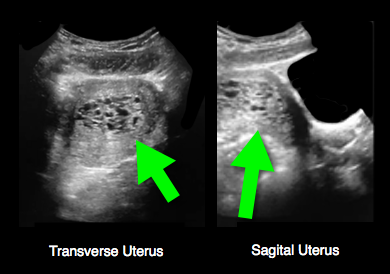
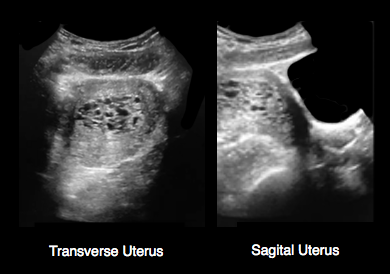
25 year-old female (G1P1) presents with 3 weeks of vaginal bleeding. Her serum beta-HCG is 65,000. Her bedside ultrasound is below; what's the diagnosis?
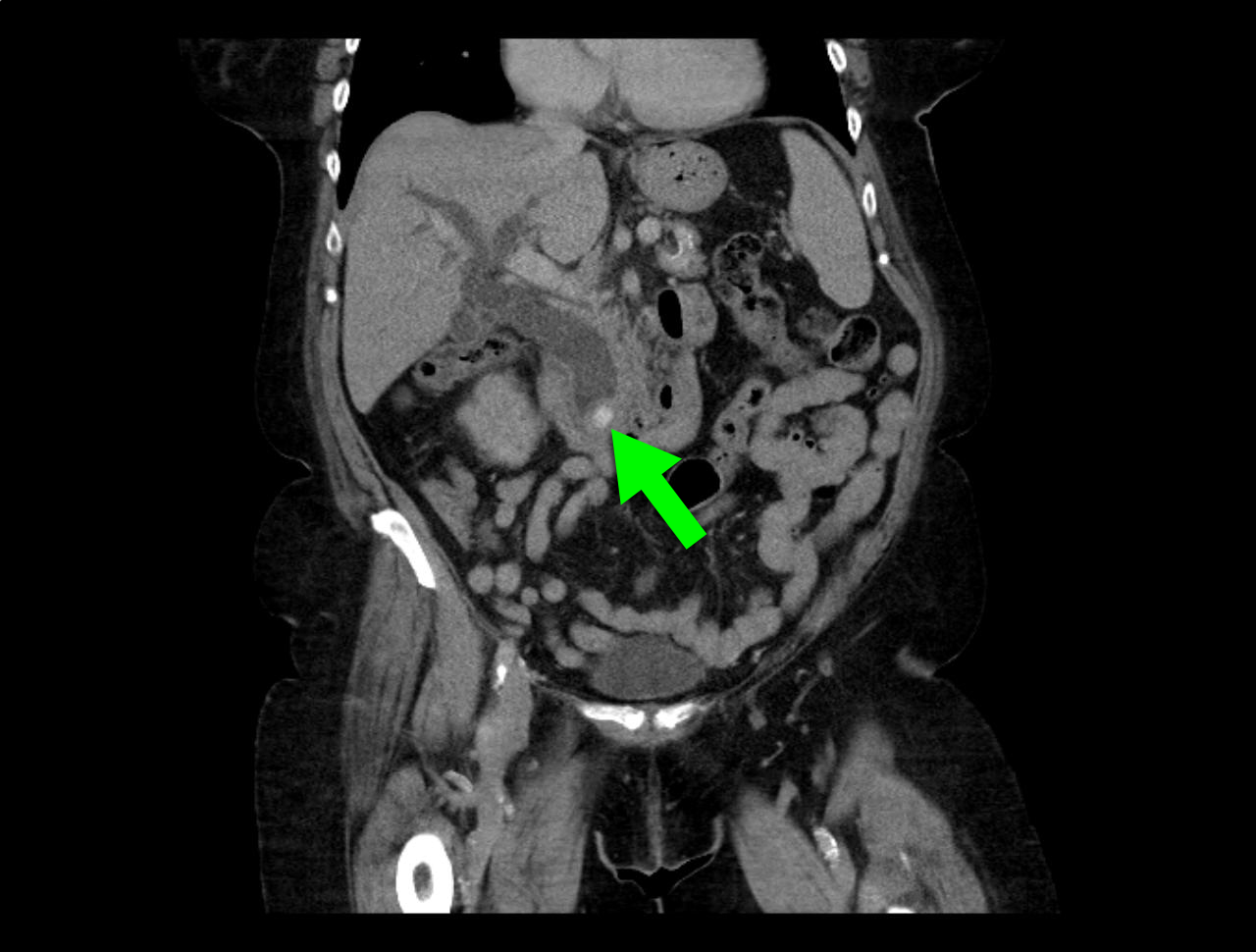
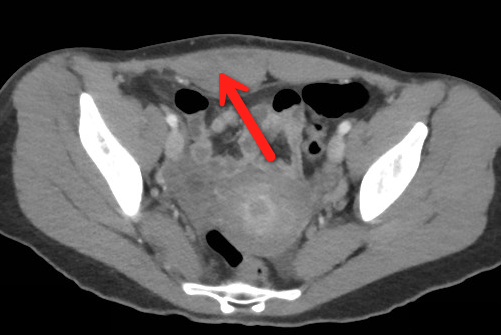
23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" pushups. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)

23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" pushups. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)
25 year-old female presents with the following. It seems to have occurred spontaneously and spontaneously resolves during her ED evaluation.

In 2001, Rivers et al. published a landmark article demonstrating an early-goal directed protocol of resuscitation that reduced mortality in septic Emergency Department patients.
Many questions have arisen throughout the years with respect to that trial; critics have complained about the overwhelming change in clinical practice based on this one single-center randomized trial.
Challenging Rivers data are the ProCESS (Protocolized Care for Early Septic Shock) investigators, who released the results from a multi-center randomized control trial of 1351 septic Emergency Department patients; the primary end-point was 60-day mortality. Click here for NEJM article.
Patients in this trial were randomized to one of three groups:
Protocol-based EGDT
Protocol-based standard (did not require central lines, inotropes, or blood transfusions
Usual care (no specific protocol; care was left to the bedside clinicians)
Bottom-line: The investigators did not find any difference in mortality between patients in the three groups and comment that the most important aspects of managing the septic patient may be prompt recognition and early treatment with IV fluids and antibiotics.
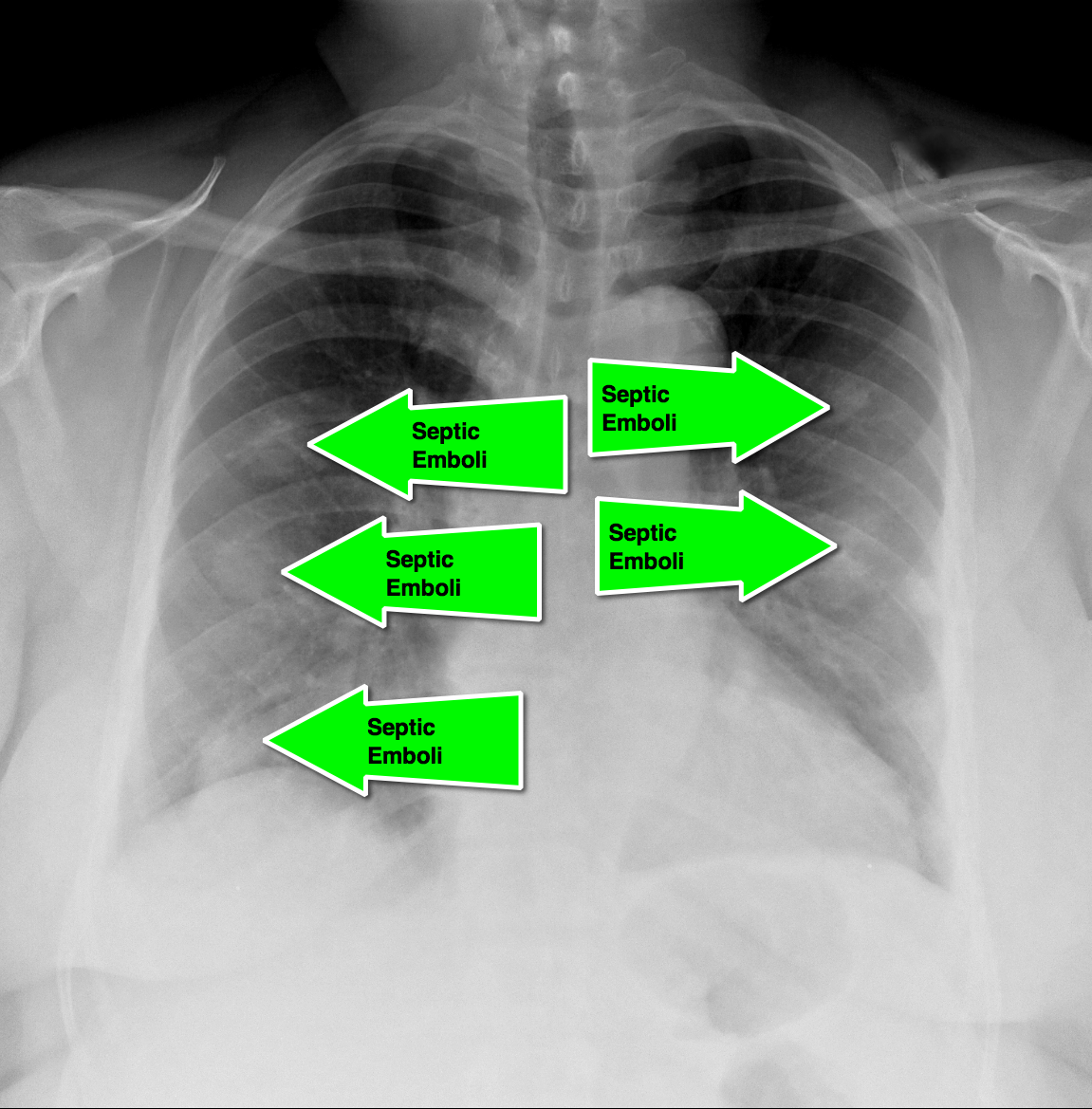
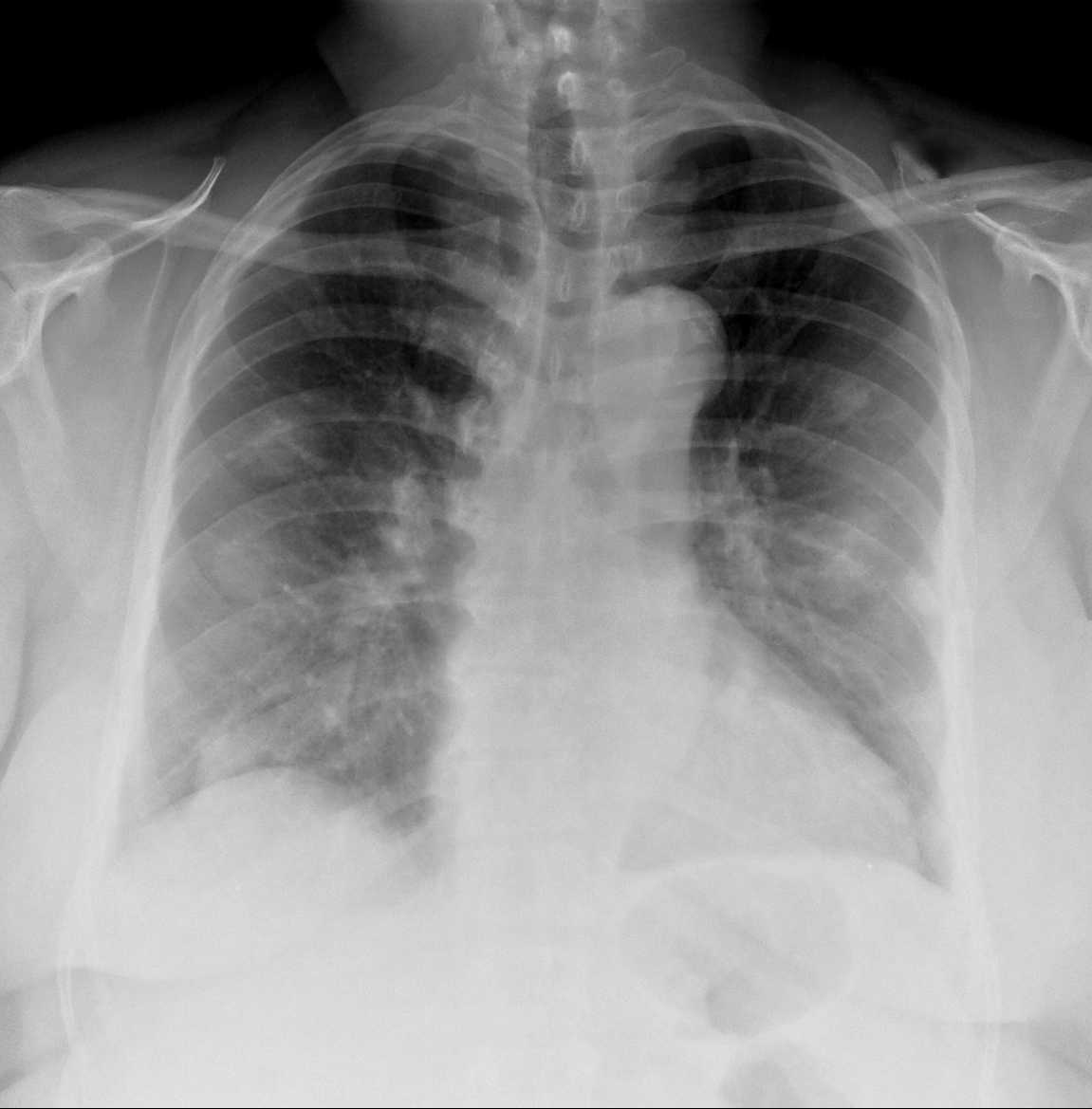
62 year-old male presents with weakness, chills, cough, and malaise. Recently, he had four teeth extracted but felt fine immediately after the extraction. Past medical history includes diabetes and hypertension; CXR is below. What’s the diagnosis?
35 year-old carpet-layer presents with swelling of the superior portion of his knee that has progressively gotten worse over one week. He has no fever and has full range of motion (although pain is worse with movement). The knee is not tender to touch and the area is not erythematous or warm. What's the diagnosis?

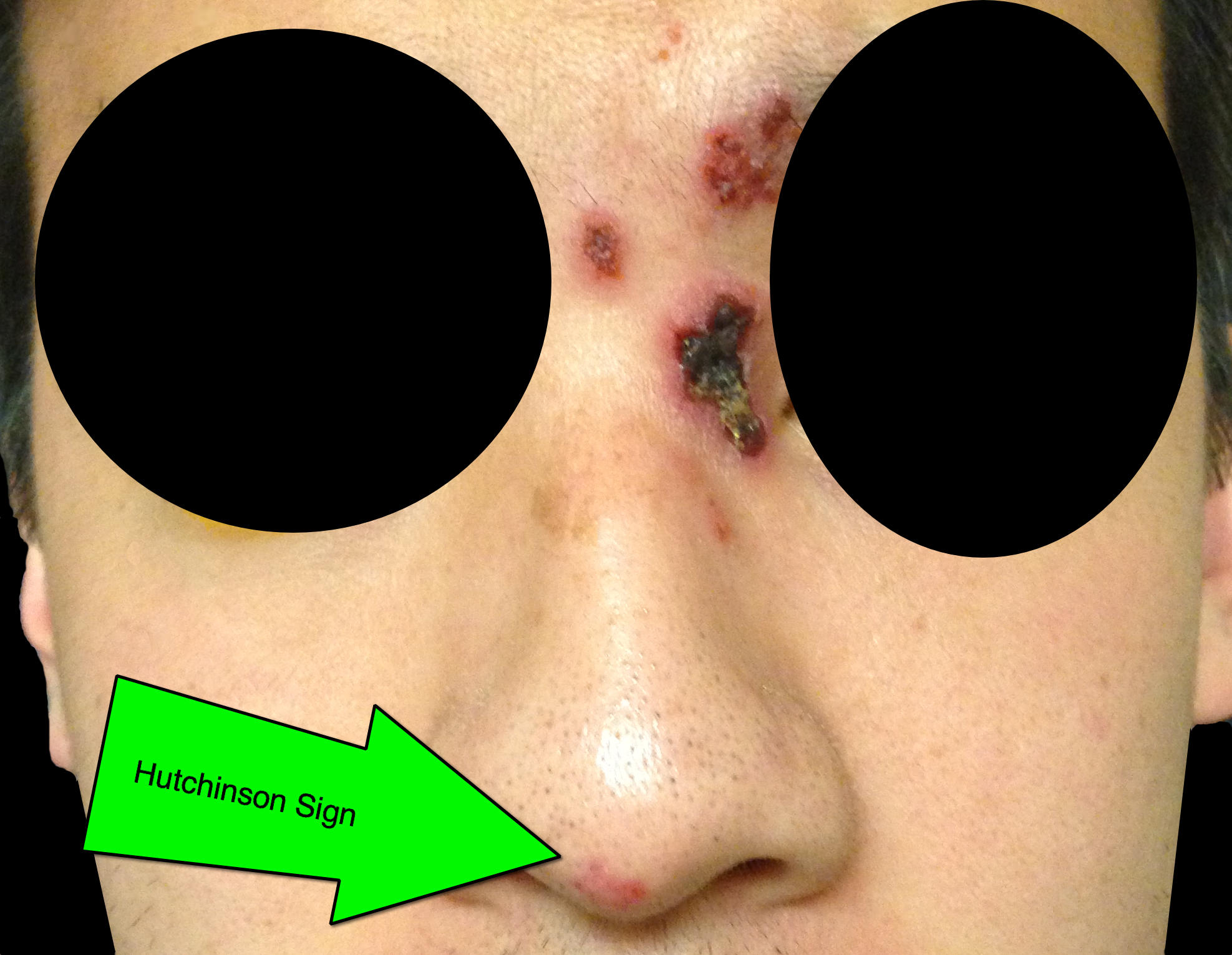
32 year-old male presents with the following. What's the diagnosis?

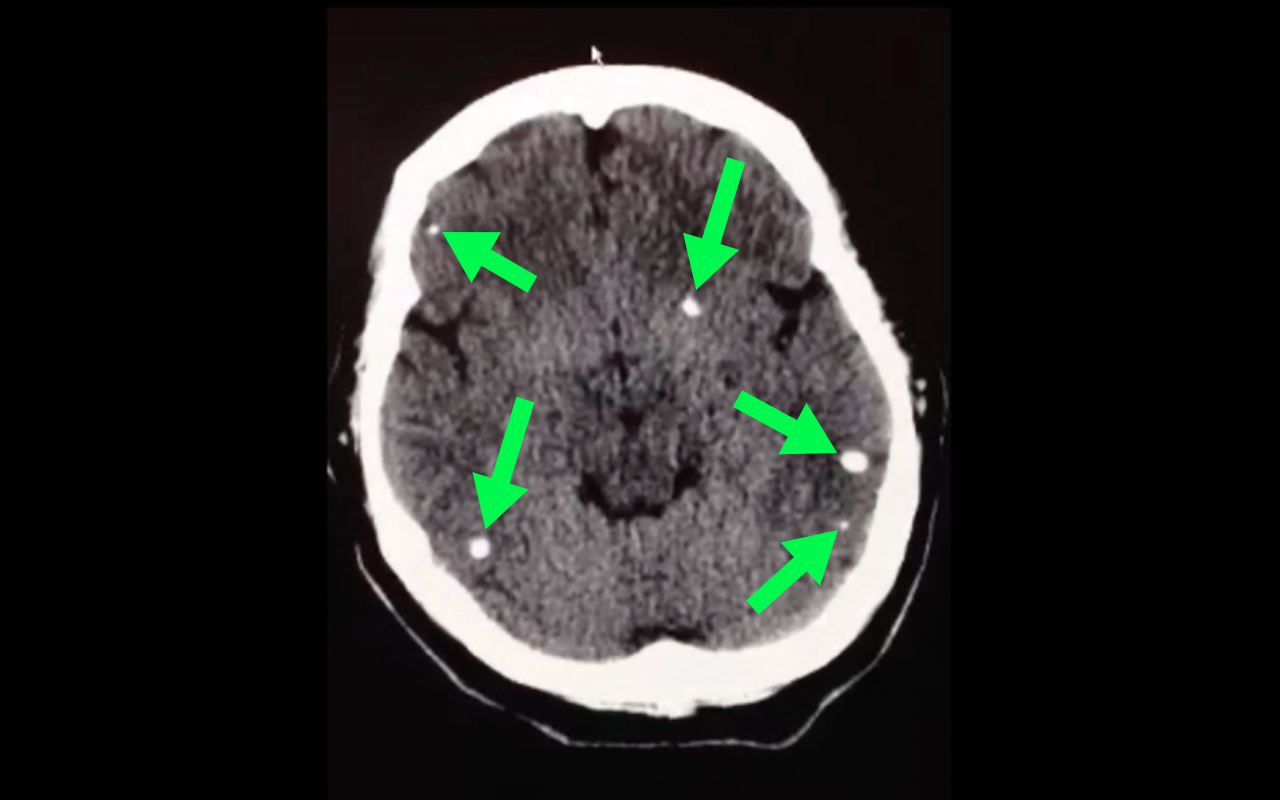
50 year-old with facial weakness and dysarthria. What's the diagnosis?
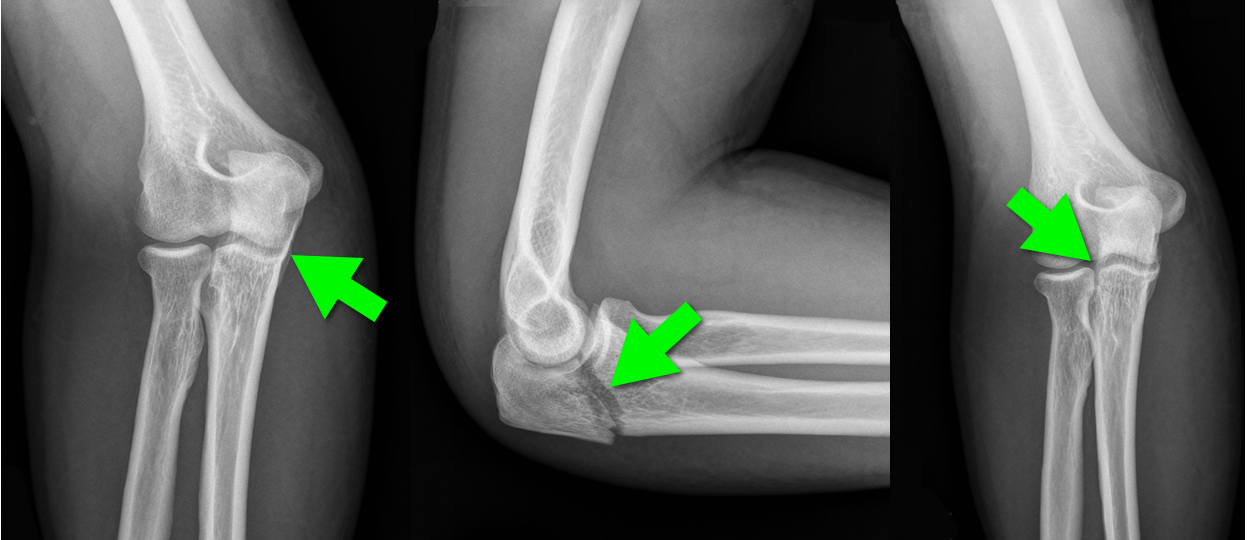
44 year-old construction worker fell off a ladder and presents with elbow pain. What's the diagnosis and what is the most commonly associated nerve injury?

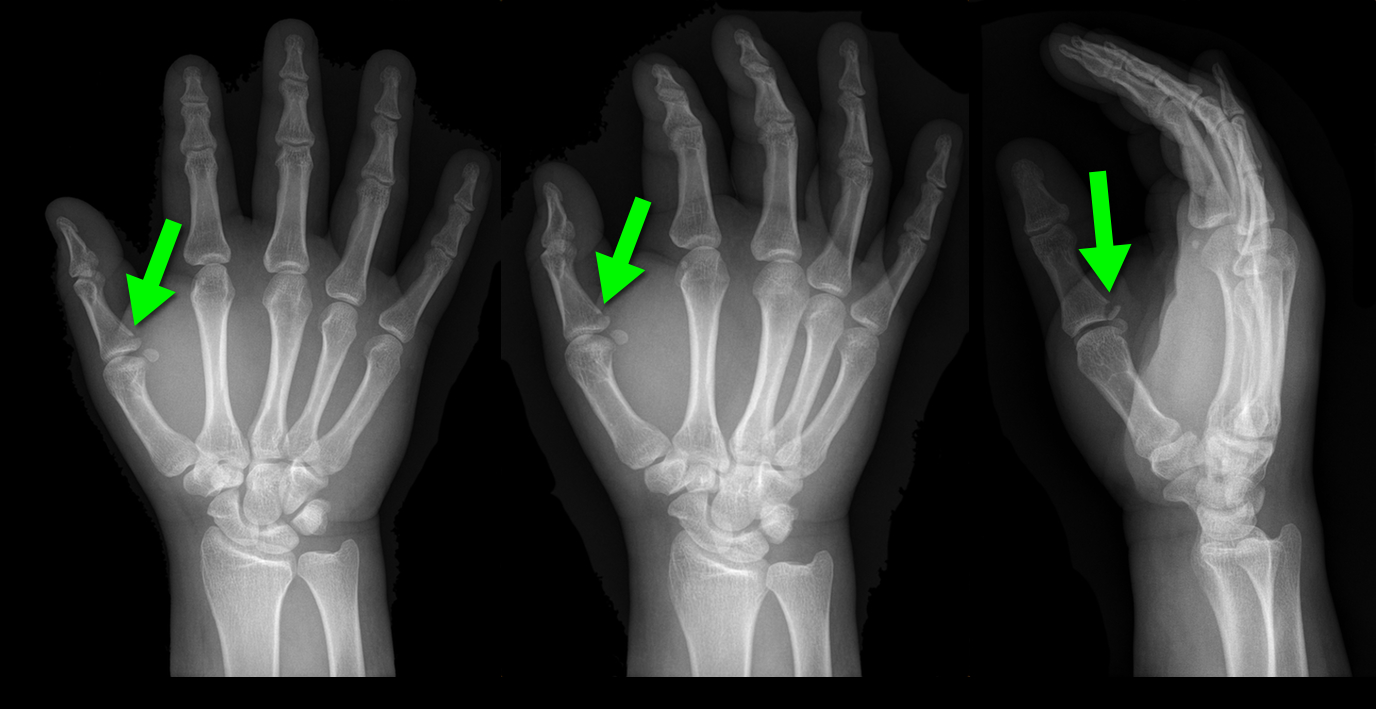
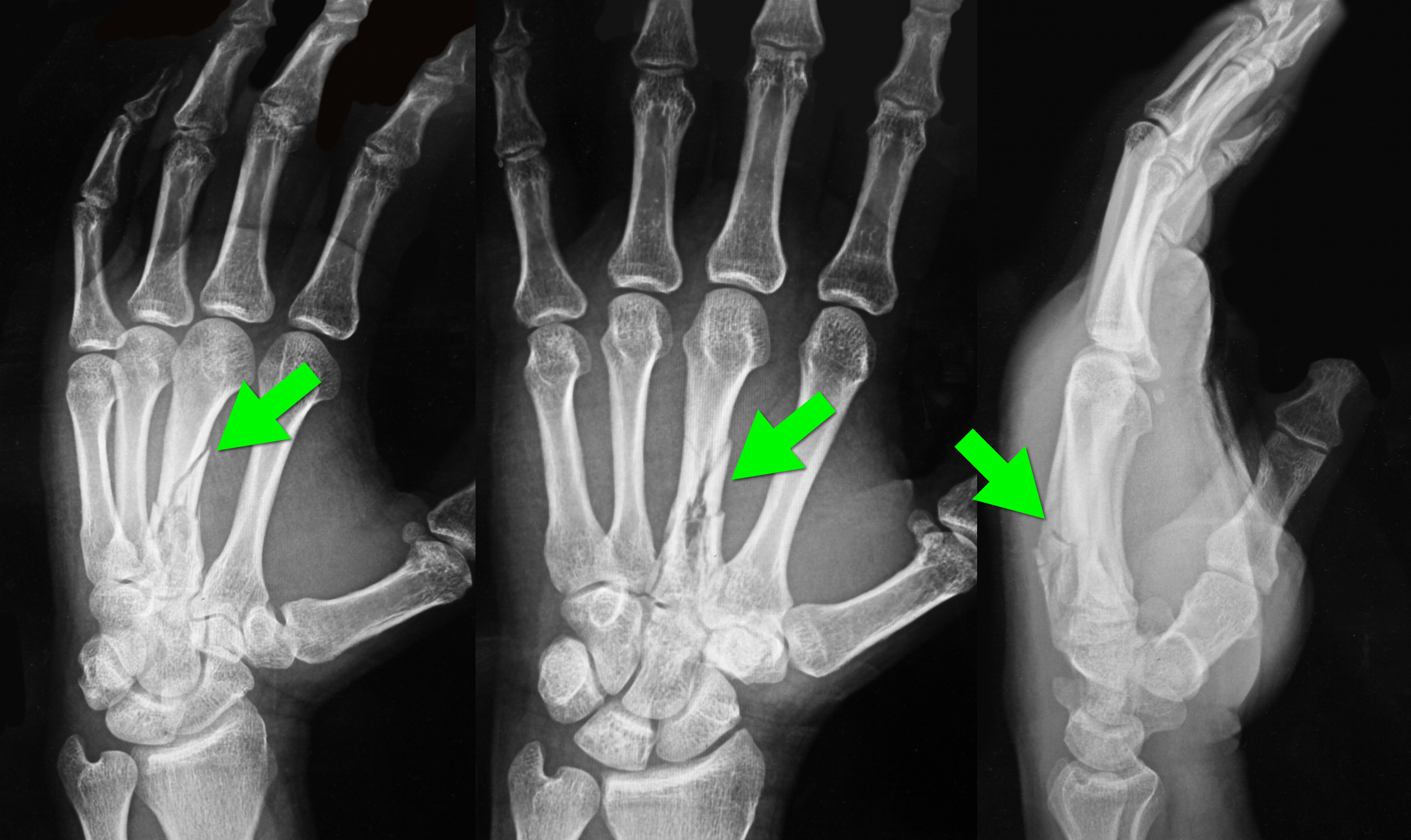
25 year-old male presents after falling off his bicycle. He complains of pain in his right-hand (he is right-hand dominant). What's the diagnosis?

34 year-old left-hand dominant male sustained injury to left hand after his pressurized greasing-gun discharged into the palm of his hand. He has a small lac to the hand but is in extreme pain. On exam his hand is very puffy and he is neurovascularly intact (XR below) What is the next step in management?

NSSTIs occur secondary to toxin-secreting bacteria; NSSTIs are surgical emergencies with a high-morbidity / mortality
Risk factors: immunocompromised host (DM, AIDS, etc.), intravenous drug use, malnourishment, peripheral vascular disease
Type I (polymicrobial; most common), Type II (monomicrobial; typically clostridia, streptococci, staph, or bacteroides), Type III (Vibrio vulnificus; seawater exposure)
Signs / Symptoms: pain out of proportion to exam (occasionally no pain at all), skin findings (blistering / bullae, gray-skin discoloration, or “Dishwater-like” discharge), or systemic toxicity (altered mental status, elevated lactate, etc.)
Diagnostic radiology
Treatment is emergent surgical debridement with simultaneous hemodynamic resuscitation PLUS broad-spectrum antibiotics; consider clindamycin becuase it has anti-toxin activity
Adjunctive therapies include Intravenous intraglobulin (neutralizes toxins secreted by bacteria) and hyperbaric oxygen
32 year-old with diabetes presents with fever, erythema, and warmth of his lower extremity; his leg is not particularly painful. He is diagnosed with cellulitis, started on antibiotics, and admitted to the hospital. While boarding in the Emergency Department he becomes rigorous and hypotensive. An ultrasound of his cellulitis is performed and is shown below. What’s the diagnosis?