Title: What's the Diagnosis? Images submitted by Dr. Joy Kay
Category: Visual Diagnosis
Posted: 8/8/2011 by Haney Mallemat, MD (Updated: 8/8/2011)
Question
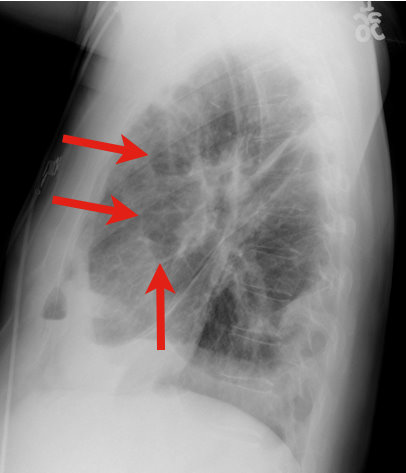
13 year-old right-hand dominant male following assault with blunt object. Diagnosis?


Show Answer
Answer: Monteggia fracture
Monteggia Fracture
- Ulnar fracture with dislocation of proximal radioulnar joint (often subtle); do not confuse with Galeazzi fracture (radial-shaft fracture with distal radioulnar dislocation)
- Due to fall on outstretched hand with arm in hyper-pronation or with direct trauma to forearm as in defensive wounds (e.g., nightstick injury).
- Ulnar fracture typically the proximal third (although any portion can be involved).
- Relatively uncommon; 1-2% forearm fractures
- Interosseous membrane (between radius and ulna) transmits forces to radioulnar joints and causes associated dislocations.
- Suspected forearm fractures should always include Xray of the wrist, forearm, and elbow
- Bado classification system (Type I-IV) used; based on displacement of radial head.
- Children may be treated with closed reduction and immobilization; adults usually require open reduction and internal fixation.
- Radial head dislocations should be reduced within 6-8 hours as can lead to articular damage and/or nerve injury.
- Radial, ulnar and/or median nerve neuropraxias (motor or sensory deficits) may complicate injury with resolution over several weeks.
Show References
Bruce H.E., Harvey J.P., Wilson J.C. Monteggia Fractures. J Bone Joint Surg Am. 1974;56:1563.
Reckling F.W. Unstable fracture-dislocation of the forearm (Monteggia and Galeazzi lesions). J Bone Joint Surg Am. 1982;64:857.
http://emedicine.medscape.com/article/1231438-overview
Follow me on Twitter (@criticalcarenow) or Google+ (+haney mallemat)