Title: What's the Diagnosis?
Category: Visual Diagnosis
Posted: 4/30/2012 by Haney Mallemat, MD (Updated: 4/30/2012)
Question
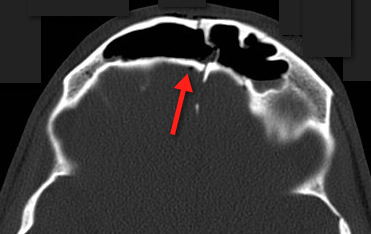
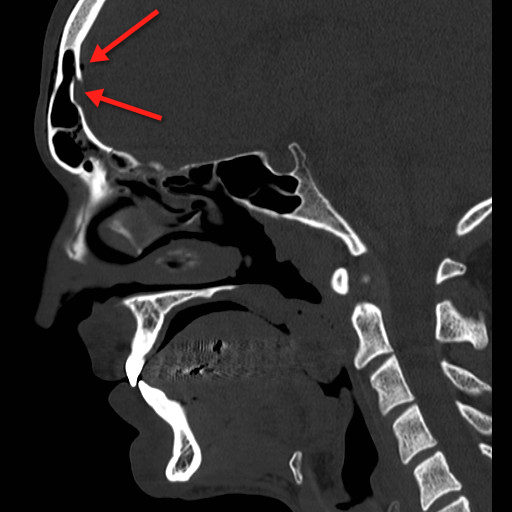
68 yo man presents with new-onset seizures; his CT is shown below. What is your differential diagnosis?

Show Answer
Cerebral Ring-Enhancing Lesions
Neoplasm
- Primary brain tumor
- Primary CNS lymphoma
- Metastatic disease
Infectious
- Pyogenic abscess
- Tuberculoma
- Syphilis
- Neurocysticercosis
- Toxoplasmosis
- Nocardiosis
- Cryptococcosis
- Aspergillosis
Neurologic
- Multiple sclerosis (lesions within the white matter)
- Sacroidosis
- Vasculitis
- Aneurysm
- Resolving hematoma
- Cerebral infarct
- Postoperative change

Bonus pearl: Do you like Emergency Ultrasound and want a quick review before you scan your next patient? Well, check out the "One-minute Ultrasound App". It's provides a quick review for many essential ultrasound studies...and yes, it's FREE for both iphone and android.
Iphone: http://itunes.apple.com/us/app/one-minute-ultrasound/id512301845?mt=8&ls=1
Garg, R., Sinha, M. Multiple ring-enhancing lesions of the brain. J Postgrad Med. 2010 Oct-Dec; 56(4):307-16
Follow me on Twitter (@criticalcarenow) or Google+ (+haney mallemat)