Although MRI is more sensitive for identifying tumors of the CNS, CT is usually the first line imaging modality in the ED. Some pearls:
- Hyperattenuation = bright = dense (blood)
- Hypoattenuation = dark = radiolucent (fluid, air, lipid, scar)
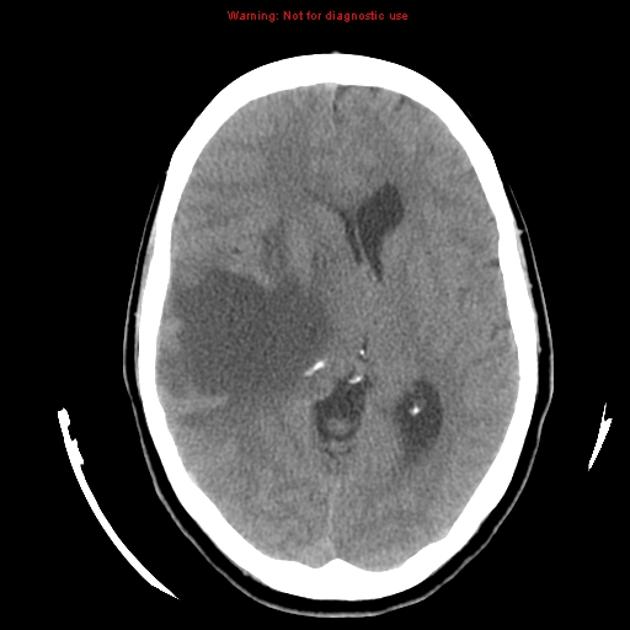
- Masses that are darker + increased volume or mass effect = edema (image 1)
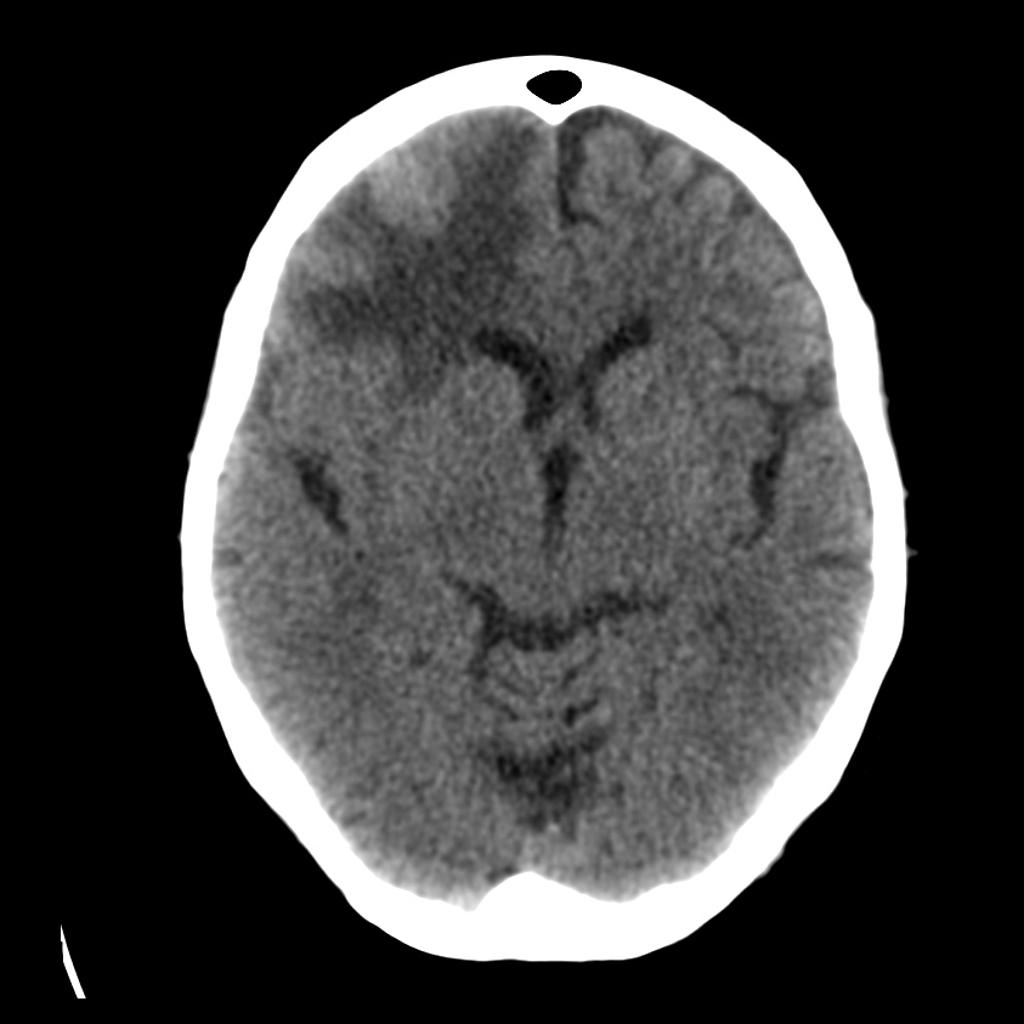
- Masses that are darker + decreased volume = scar tissue or atrophy (image 2)
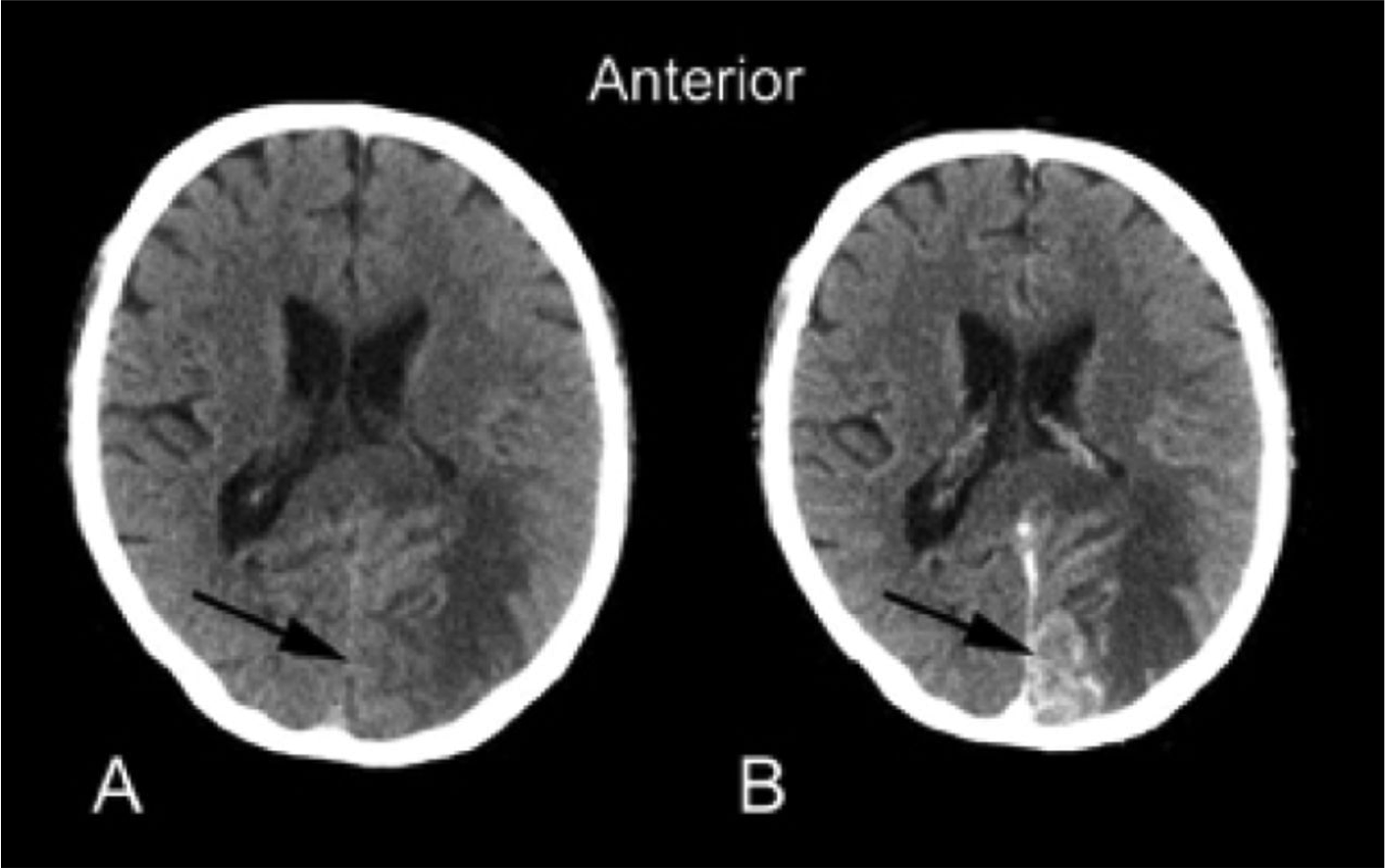
- Masses that are bright + edema = hemorrhage (image 3)
- Adding IV contrast improves detection of tumors: abnormal enhancement from disruption of blood brain barrier, necrosis or increased vascularity. (Image 4)