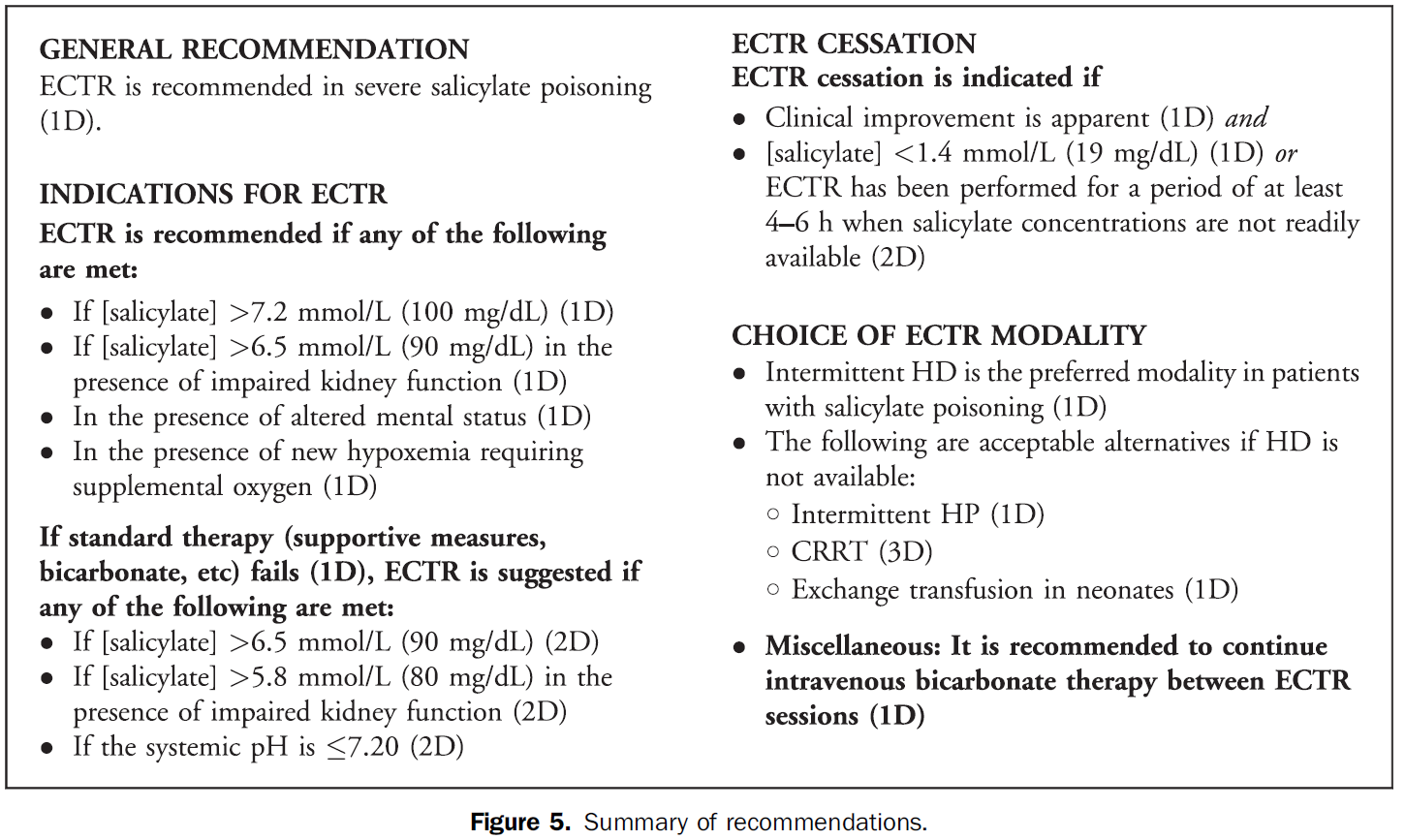
The Extracorporeal Treatments in Poisoning (EXTRIP) Workgroup has published their latest review, this time on extracorporeal treatment for salicylate poisoning. Here are their recommendations on when to dialyze:
Flumazenil is generally avoided in most adult patients with suspected benzodiazepine overdose due to resedation, seizures/withdrawal, inconsistent reversal of respiratory depression, and the potential for proconvulsant coingestants.
Three relatively recent poison center studies have attempted to demonstrate the safety of flumazenil in this setting. [1-3] In the first study there were 904 adult patients with 13 reported seizures and 1 death. [1] A second study specific to pediatric patients reported 83 patients with no seizures and no deaths. [2] A third study found 80 patients with 1 seizure and 0 deaths. [3]
On the surface, it may appear that flumazenil is safe to give. But, retrospective poison center studies from voluntary reporting cannot be used to prove a drug's safety. The true denominator is unknown. In the pediatric study, we wouldn't expect children to experience withdrawal since they aren't on chronic benzodiazepine therapy. [2] So, it's no surprise there weren't any seizures or deaths.
A recent systematic review and meta-analysis of randomized trials summed it up perfectly: "Flumazenil should not be used routinely, and the harms and benefits should be considered carefully in every patient." [4] Cases in which to consider flumazenil are pediatric patients and reversal of procedural sedation if needed.
How much does the blood glucose concentration increase when dextrose 50% (D50) is administered?
A new study found a median increase of 4 mg/dL (0.2 mmol/L) per gram of D50 administered.
This retrospective study was conducted in critically ill patients who experienced hypoglycemia while receiving an insulin infusion. While it may not directly apply to all Emergency Department patients, an estimation of the expected blood glucose increase from rescue dextrose is helpful. If the blood glucose doesn't respond as anticipated, it can help us troubleshoot possible issues (eg, line access).
The New England Journal of Medicine and Lancet both published studies evaluating idarucizumab for reversal of dabigatran. It is a monoclonal antibody fragment that binds dabigatran with high affinity. Dr. Ryan Radecki summarizes the two articles on his EM Lit of Note blog.
Here are a few take home points from these early studies:
Transitioning Diabetic Ketoacidosis (DKA) patients off an insulin infusion can be challenging. If a long-acting insulin, such as glargine or levemir, is not administered at the correct time to provide extended coverage, patients can revert back into DKA.
Pilot Study
A prospective, randomized, controlled pilot study in 40 patients evaluated administration of glargine within 2 hours of insulin infusion initiation compared to waiting until the anion gap (AG) had closed.
What they did
What they found
Mean time to closure of AG, mean hospital LOS, incidents of hypoglycemia, rates of ICU admission, and ICU LOS were all similar between the groups.
Application to Clinical Practice
Although just a pilot study (using a convenience sample), early glargine administration seemed to be absorbed adequately (based on time to AG closure) and was not associated with increased risk of hypoglycemia. If confirmed in a larger study, this technique could help optimize care of DKA patients in the ED by eliminating the often-mismanaged transition step later on.
The Extracorporeal Treatments in Poisoning (EXTRIP) Workgroup has published their latest review, this time on extracorporeal treatment for salicylate poisoning. Here are their recommendations on when to dialyze:
Vancomycin guidelines recommend an initial dose of 15-20 mg/kg based on actual body weight (25-30 mg/kg in critically ill patients). [1] The MRSA guidelines further recommend a max dose of 2 gm. [2]
But, what dose do you give for an obese patient that would require more than 2 gm?
A new study provides some answers to this question. [3] Obese-specific, divided-load dosing achieved trough concentrations of 10 to 20 g/mL for 89% of obese patients within 12 hours of initial dosing and 97% of obese patients within 24 hours of initial dosing.
Application to Clinical Practice
Caveats
The study used some more specific dosing calculations based on renal function and percentage above IBW. If patient's renal function is abnormal, consultation with a pharmacist is recommended.
In addition to the down regulation of GABA receptors in chronic ethanol users, there is an upregulation in NMDA receptor subtypes. Although the pathophysiology is much more complex, when ethanol abstinence occurs, there is a shortage of GABA-mediated CNS inhibition and a surplus of glutamate-mediated CNS excitation. If GABA agonists are the mainstay of treatment, why not also target the NMDA receptor? Enter ketamine.
Only one study exists and was published recently.
While the dexmedetomidine studies should not be using reduction in benzodiazepine requirements as an endpoint, it may be acceptable for ketamine since it actually works on the underlying pathophysiology. More studies are needed but it's good to see we’re starting to look at it.
Aside from sodium chloride and sodium bicarbonate, several commonly used emergency department medications (namely IV antibiotics) contain a significant amount of sodium. In patients with heart failure or other conditions requiring sodium restriction, judicious use should be considered.
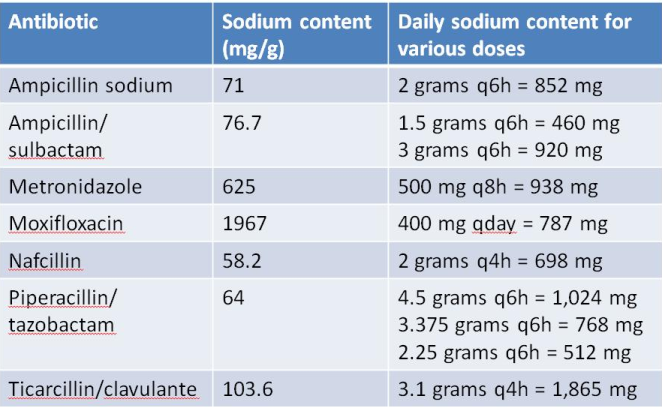
Notes:
A new study from South Korea identified 3 potential clinical predictors of developing delirium tremens in patients presenting to the ED with alcohol withdrawal seizures.
If one or more is present, these findings may help assess alcohol withdrawal patients for the risk of developing DTs.
Application to Clinical Practice
For many institutions, clindamycin is not as good as it used to be for methicillin-resistant Staph aureus (MRSA). When treating skin and soft tissue infections (SSTI), this can be challenging. Clindamycin still covers skin strep species very well, but not always the staph. On the other hand, trimethoprim-sulfamethoxazole (TMP-SMX) covers staph really well, but not so much the strep.
What They Did
A new double-blind, multicenter, randomized study in NEJM compared these two antibiotics in 524 patients with uncomplicated skin infections who had cellulitis, abscess larger than 5 cm, or both. All abscesses underwent incision and drainage. The primary outcome was clinical cure rate 7-10 days after the end of treatment.
What They Found
There was no difference in clinical cure rate between the two groups (80.3% for clindamycin, 77.7% for TMP-SMX).
Problems with the Study
Application to Clinical Practice
Unknown. This study seems to suggest TMP-SMX might be ok in uncomplicated cellulitis even though we assume strep species are the causitive organism. However, we already know cephalexin is equivalent to cephalexin + TMP-SMX from the 2013 study by Pallin et al. Why not just use cephalexin which has less adverse effects than TMP-SMX?
With such low clindamycin resistance, even to the staph species, perhaps that is why the two treatments were similar. Also, why did successfully drained abscesses need antibiotics? Finally, there were many exclusion criteria which eliminated many of the patients we see in the ED.
For a different, critical perspective of this NEJM study, Dr. Ryan Radecki gives his thoughts on his EM Lit of Note blog.
In the midst of an unprecedented opioid epidemic, there have been considerable efforts to expand access to naloxone (Doyon S, et al. J Med Toxicol 2014;10:431-4). If the situation arises when you need to write a prescription for it, here's how:
Option 1: Naloxone vial and needle traditional IM/SQ using 0.4 mg/mL injection vial and needles (least expensive $40, FDA approved)
Naloxone 0.4 mg/mL single dose vial and 3 cc, 23 g, 1 inch syringes, #2 each
SIG: Inject 1 mL intramuscularly upon signs of opioid overdose. May repeat X 1. Call 911.
Option 2: IMS/Amphastar 2 mg/2 mL prefilled syringe and mucosal atomization device ($95/kit, products FDA approved but intranasal administration is off-label)
Naloxone 2 mg/2 mL prefilled syringe and intranasal atomizer device, #2 each
SIG: Spray one-half of syringe (1 mL) into each nostril upon signs of opioid overdose. May repeat X 1. Call 911.
Option 3: Evzio Autoinjector ($200-700 per Rx though many insurances cover it and the company has vouchers available, FDA approved in 2014, evzio.com/hcp)
Evzio 0.4 mg, #1 two-pack
SIG: Use as directed upon signs of opioid overdose. May repeat X 1. Call 911.
Emergency Departments are increasingly searching for alternatives to opioids for acute pain management.
An urban trauma center in California retrospectively evaluated their use of low-dose ketamine for acute pain over a two-year period. [1]
Application to Clinical Practice
There was no comparison group and there was no mention of what other pain medicines were given. Adverse events are often under-reported in retrospective studies. This study seems to demonstrate that low-dose ketamine administration for acute pain management in the ED is feasible with a low rate of adverse effects.
It's worth noting that a new review of 4 randomized controlled trials evaluating subdissociative-dose ketamine found no convincing evidence to support or refute its use in the ED. The 4 included trials had methodologic limitations. [2]
A new review summarized published adverse effects when IV lipid emulsion is used along with venous-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiotoxic drug poisoning.
Not surprisingly, running fat through the ECMO circuit can cause some issues. Here's what's been published:
It's unclear how these findings should change management if using both treatment modalities, but at the very least, be aware that fat depostion in the VA-ECMO circuits and increased blood clot formation can occur.
We know vancomycin should be dosed based on weight rather than the default 1 gm dose so many patients receive. A past Academic Life in EM post explores the nuances of proper vancomycin dosing. But do higher loading doses in the ED actually lead to more therapeutic trough levels?
New Data
A new randomized trial compared ED patients receiving 30 mg/kg initial doses vs. 15 mg/kg. [1] There was a significantly greater proportion of patients reaching target trough levels of 15 mg/L at 12 hours among the patients who received a 30 mg/kg loading dose as compared with a traditional 15 mg/kg dose (34% vs 3%, P < 0.01). This study did not use a max dose of 2 gm. They included patients up to 120 kg who received 3.6 gm loading doses! Patients with creatinine clearance < 50 mL/min were excluded. There was no difference in incidence of nephrotoxicity between the groups.
Application to Clinical Practice
Application to Clinical Practice
WBI can facilitate removal of select toxicants from the gastrointestinal tract in some patients, but there is no convincing evidence from clinical studies that it improves the outcome of poisoned patients.
Does IV magnesium have a role in the management of acute migraine headache in the ED? A new study says yes. [1]
Intervention
What They Found
Magnesium sulfate was more effective in decreasing pain severity at 20-min (pain scale 5.2 vs. 7.4) and 1-h (2.3 vs. 6.0) and 2-h (1.3 vs. 2.5) intervals after treatment (p < 0.0001) compared to treatment with dexamethasone/metoclopramide.
Should beta blockers be withheld in cocaine-chest pain patients?
A new study retrospectively compared patients who received beta blockers as an inpatient to those who did not. Even though the beta blocker group had higher risk clinical characteristics, there was no difference in the composite primary end point of myocardial infarction, stroke, ventricular arrhythmia, or all-cause mortality within 24 hours of beta blocker use.
Important Limitations
The potentially dangerous interaction between beta blockers and cocaine is likely a much larger issue in patients with very recent cocaine use in the setting of a catecholamine surge. A retrospective analysis likely doesn't include those patients.
Application to Clinical Practice
While this study doesn't answer the question about beta blocker use in acute cocaine toxicity, it does provide some reassurance about the safety of beta blockers given for cocaine-related chest pain.
Many of the oral antibiotics prescribed in the ED have good bioavailability. So, a one-time IV dose before discharge generally won't provide much benefit.
In fact, a new prospective study found that a one-time IV antibiotic dose before ED discharge was associated with higher rates of antibiotic-associated diarrhea and Clostridium difficile infection. [1] One-time doses of vancomycin for SSTI before ED discharge are also not recommended (see Academic Life in EM post).
Bottom Line
Though there are a few exceptions, if a patient has a working gut, an IV dose of antibiotics before ED discharge is generally not recommended and may cause increased adverse effects. An oral dose is just fine.
A new population-based case-control study in older adults has linked the administration of trimethoprim-sulfamethoxazole (Bactrim, TMP-SMX) to increased risk of sudden death in patients also receiving angiotensin converting enzyme inhibitors (ACE-I) or angiotensin receptor blockers (ARB). [1]
Hyperkalemia is the suspected cause. [2] Compared to amoxicillin, TMP-SMX was associated with an increased risk of sudden death (adjusted odds ratio 1.38, 95% confidence interval 1.09 to 1.76) within 7 days of exposure to the antibiotic.
Practice Change
In older patients receiving ACE-Is or ARBs, TMP-SMX is associated with an increased risk of sudden death. When appropriate, alternative antibiotics should be considered.
The cross-reactivity between cephalosporins and penicillins is significantly lower than the 10% figure many of us learned. In fact, the beta-lactam ring is rarely involved. So, when the warning pops up next time you order ceftriaxone in a penicillin-allergic patient, what should you do?
In a patient with a documented penicillin allergy, here is a simple chart to help determine when a cephalosporin is ok to use:
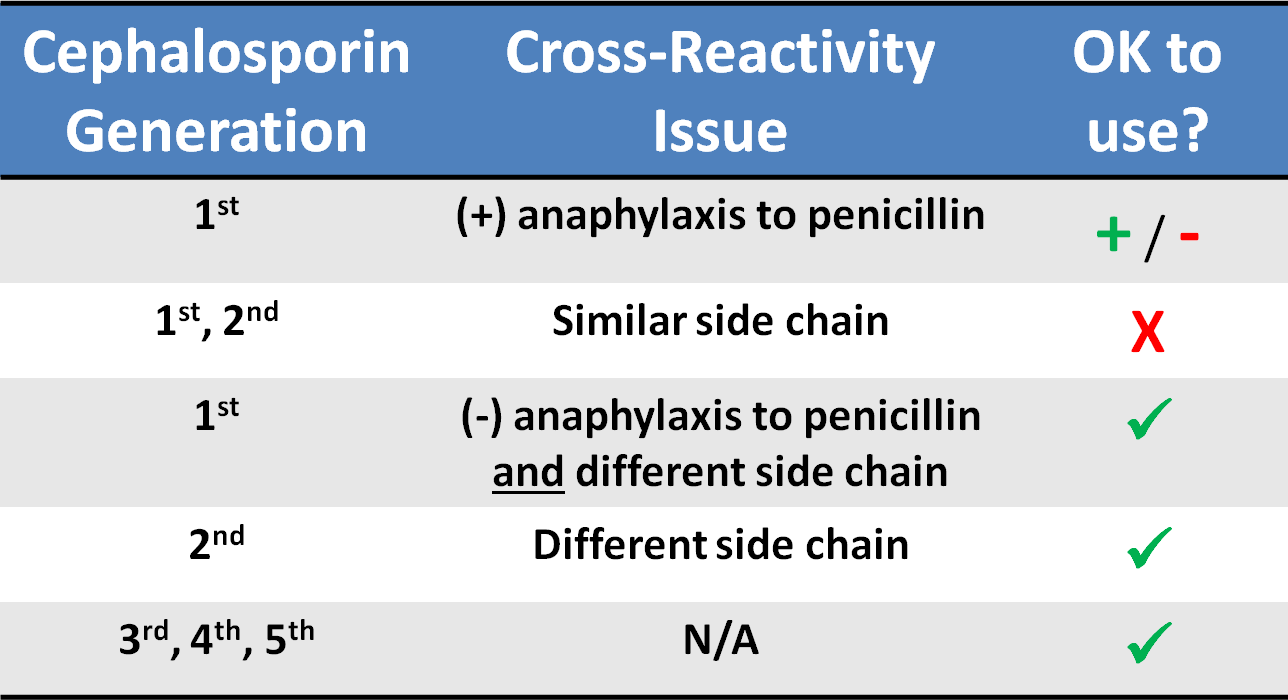
Common penicillins and cephalosporins with similar side chains include ampicillin/amoxicillin and cephalexin, cefaclor, cephadroxil, and cefprozil.