Injury was originally described as an occupational hazard in Scottish gamekeepers (from breaking the necks of rabbits against the ground). Today, skiing is now the most common cause and injury is now the second most common orthopedic injury in skiers (MCL injury #1).
Injury to the ulnar collateral ligament (UCL) results from a sudden forced abduction (radial deviation) stress at the MCP joint of the thumb, commonly due to a fall against a ski pole or the ground.

http://blog.fitter1.com/wp-content/uploads/2010/04/b_14_1_2a.jpg
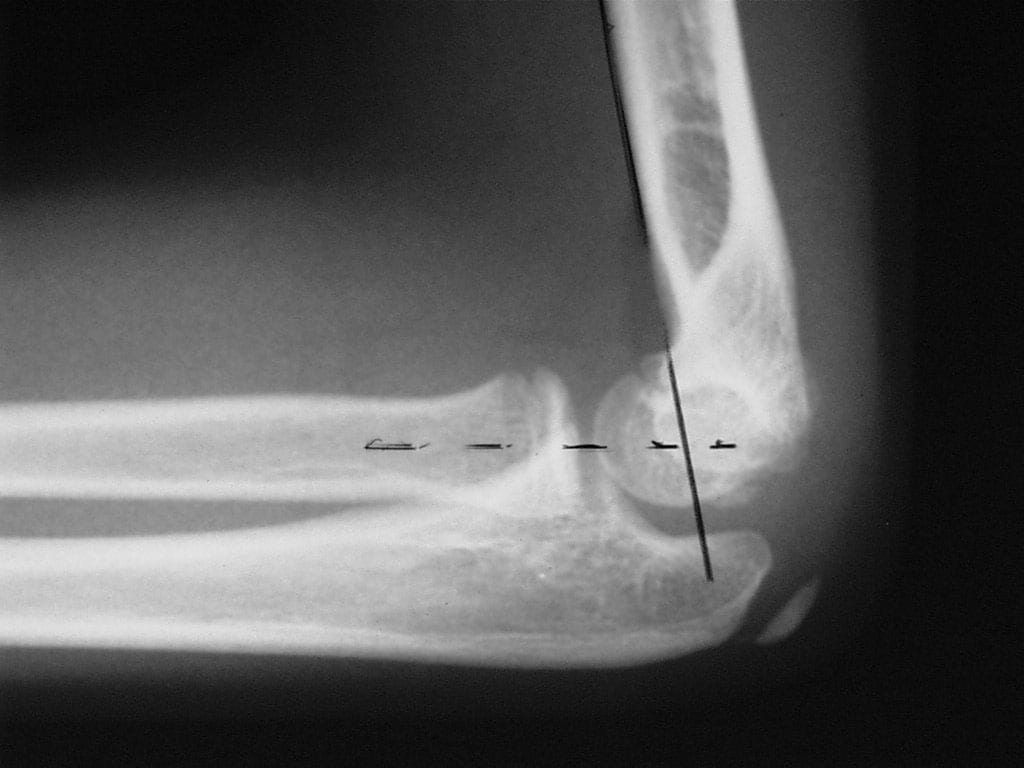
The most frequent site of rupture is the insertion into the proximal phalanx. The UCL may even avulse a small portion of the proximal phalanx at its insertion site.

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652013.jpg
Consider imaging before stress testing (to avoid further displacing a fracture)

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652060.jpg
Stabilize in a thumb spica splint and refer to hand surgery.
Calling this entity a “simple sprain” may result in chronic disability (chronic pain, instability, loss of pinch strength)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}