Acute brachial plexus neuritis is an uncommon disorder that is easily confused with cervical radiculopathy.
Patients present with a characteristic pattern of acute onset of burning pain. Pain subsides in days to weeks and is then followed by profound weakness and muscle wasting changes affecting the shoulder and upper extremity. Weakness is best identified in the deltoid, biceps and rotator cuff muscles. Strength gradually recovers over 3-4 months.
DDX: The constellation of pain, weakness and sensory loss associated with cervical radiculopathy tend to occur simultaneously. Also cervical radiculopathy tends to involve only a single root.
ED treatment is with analgesics and physical therapy and PCP referral for outpatient MRI/EMG. Consider a sling in those with severe shoulder weakness.
Refractory Osteomyelitis is defined as a chronic osteomyelitis that persists or recurs after appropriate interventions have been performed or where acute osteomyelitis has not responded to surgery and antibiotics.
Case series, animal data and non-randomized prospective trials suggest that the addition of Hyperbaric Oxygen therapy to routine surgical and antibiotic management of previously refractory osteomyelitis is safe and improves the rate of infection resolution.
In patients with osteomyelitis involving spine, skull, sternum, HBOT is recommended prior to surgical intervention.
Typically patients require 20-40 daily dives for sustained therapeutic benefit.
How does HBOT work in osteomyelitis?
1. Restoration of normal to elevated O2 level in infected bone.
2. Leukocyte mediated killing of aerobic bacteria is restored when low O2 tension intrinsic to osteomyolitic bone is restored to physiologic or supra-physiologic levels.
3. HBOT is noted to exert direct suppressive effects on anaerobic infections.
4. HBOT augment the transport of certain abx (aminoglycosides and cephalosporins) across bacterial cell wall.
5. Enhance osteogenesis
6. Enhance angiogenesis
thank you to Dr. Sethuraman for this pearl
Emergency physicians are often called upon to provide event coverage for marathons.
Prolonged endurance racing is safe for the majority of participants.
Hyponatremia (8.2% - 13.5%) - finishing times of greater than 4 hours is an independent risk factor
Hypokalemia – uncommon
Renal function – BUN > 30 or Cr > 1.4 mg/dL (23.6%). There is no data that this is of any clinical significance.
Cardiac Troponin - (11%) had significant increases (troponin T > or = 0.075 ng/mL or troponin I > or = 0.5 ng/mL). Elevations were more commonly seen with weight loss and increased Cr levels and may be associated with running inexperience (< 5 previous marathons) and young age (< 30 years) though interestingly not with race duration or traditional cardiac risk factors.
Findings are similar for men and women
Pes Anserine Bursitis is an inflammatory condition of the medial knee
Occurs at the bursa of the pes anserinus which overlies the attachment of the 1) Sartorius 2) gracilis and 3) semitendinosis tendons
Note the location is 2-3 inches below the knee joint on the medial side
http://kneespecialistsurgeon.com/images/uploaded/Pes%20anserinus%20bursitis%20image.jpg
http://eso-cdn.bestpractice.bmj.com/best-practice/images/bp/en-gb/575-27_default.jpg
Patients complain of pain (especially with stair climbing)
PE: Tenderness to palpation of the bursa with mild swelling
DDx: MCL tear, medial meniscus injury, medial (knee) compartment arthritis
Treatment: Cessation/modification of offending activities, Icing and ice massage, NSAIDs, hamstring stretching and physical therapy. Failure of the above should prompt referral for bursal steroid injection.
Kienbock’s disease is a rare entity involving collapse of the lunate due to avascular necrosis and vascular insufficiency.
Occurs most commonly in young adults aged 15 to 40 years.
Cause is unknown but believed to be due to remote trauma or repetitive microtrauma in at risk individuals.
Patients complain of wrist pain, stiffness and swelling
On exam, limited range of motion, decreased grip strength and passive dorsiflexion of the 3rd digit produces pain.
Dx: plain film in the ED and with MRI as an outpatient.
Tx: Wrist immobilization with splint and refer to orthopedics. Ultimate treatment is individualized and there is no clear consensus.
Lunate sclerosis seen on plain film
http://orthoinfo.aaos.org/figures/A00017F02.jpg
AVN of the lunate seen on MRI
http://www.assh.org/Public/HandConditions/PublishingImages/KeinbocksMRI_figure3.JPG
Transient brachial plexopathies aka Burners and Stingers
Brachial plexus injuries are the most common peripheral nerve injuries seen in athletes.
49-65% of all college football players have experienced at least one burner with a 87% recurrence rate.
Injuries most commonly occur at C5-C6 but may involve any root level.
3 Mechanisms: Commonly due to
1) Traction caused by lateral flexion of the neck away from the involved side
2) Compression of the upper plexus between shoulder pads and scapula
3) Nerve compression caused by neck hyperextension and ipsilateral rotation.
CC: Burning or numbness in the neck, shoulder and/or arm
Symptoms are UNILATERAL and tend to usually last seconds to minutes
Symptoms are reproduced by the Spurling maneuver.
Function gradually returns from the proximal muscle groups to the distal muscle groups.
Because most burners are self-limited, the most important goal is to rule out an unstable cervical injury.
Meralgia Paresthetica - caused by entrapment of the lateral femoral cutaneous nerve (LFCN)
The LFCN is responsible for sensation of the anteriorlateral thigh.
http://www.chiropractic-help.com/images/Meralgia-Paresthetica.jpg
NOTE* It has no motor component!
Associated with pregnancy, wearing tight pants, belts, girdles, and in diabetic and obese patients.
Symptoms include numbness, paresthesias and pain (not weakness). Worse w walking, standing. Better w sitting.
Diagnosis is clinical but may be confirmed with nerve conduction studies
Treatment includes, NSAIDs, injection and surgery for refractory cases.
Gout treatment considerations
Treatment is directed to relieve pain and inflammation
NSAIDs, steroids and narcotics are the mainstays of treatment. All 3 should be used in combination.
Aspirin should be avoided as it may increase uric acid levels
Note: not in prevention doses (81mg) in treatment doses (325-650mg q4h)
NSAIDs and steroids take time to be effective. Provide appropriate analgesia with oral narcotic medication for short term relief
Don't forget the benefit of splinting a "hot" joint (the ankle or wrist for example)
NSAIDs: Use may be limited in the elderly and in those on coumadin or with peptic ulcer disease. 5-7 days of treatment is usually sufficient. Indomethacin is most commonly used (50 mg TID, which may be tapered to 25 mg TID after 3 days)
Steroids: Likely more effective than NSAIDs. Oral prednisolone is more effective than naproxen (1). Use prednisone 30-50 mg for 3-5 days without tapering (as we use for asthma). May be useful to supplement with NSAIDs on the tail end to prevent a rebound flare. If tapping the joint consider intraarticular steroids. If there is concern for medical noncompliance with oral steroids consider IM steroids (triamcinolone 60mg or methylprednisolone).
Gout Part 2
GOUT part 1
Gout is an inflammatory arthritis that classically affects the first metatarsal phalangeal joint
Gout prefers cool ambient temperature hence gouty tophi prefer the great toe (one of the coldest parts of the body) and avoids "warmer" joints such as the hip and shoulder.
Remember that gout can affect other joints as well (elbow, wrist, knee and ankle) and can cause painful bursitis and tendonitis
Multiple joints can be involved simultaneously (leading to confusing with RA and OA)
The involved joint will often be red, hot, swollen and very painful leading to easy confusion with cellulitis and or a septic arthritis
Diagnose gout by demonstrating monosodium urate crystals in the synovial fluid.
**Remember previous pearl by Dr. Bond regarding the coexistence of gout with septic joint**
Serum uric acid levels are commonly elevated but can be normal or even low
Use caution with this test because asymptomatic hyperuricemia is much more common than gout
Cubital Tunnel Syndrome aka Radial Tunnel Syndrome
Sever's disease ,aka calcaneal apophysitis, is a common overuse injury in the pediatric and adolescent population.
Occurs secondary to traction of the calcaneus that most often occurs in young athletes (8-12 yo)
-Avg. age of presentation is 11 years 10 months in boys & 8 years 8 months in girls
-Repetitive traction to the weaker apophysis, induced by the pull of the Achilles on its insertion
Hx: Heel pain that increases with activity (running, jumping).
-May involve one (40%) or both (60%) feet
PE: Tenderness of the posterior heel at the Achilles tendon insertion and ankle dorsiflexor weakness
Imaging: Radiography is often normal. When positive, show fragmentation and sclerosis of the calcaneal apophsis. NOTE: These findings are nonspecific and also are observed in asymptomatic feet.
http://t0.gstatic.com/images?q=tbn:ANd9GcQ9R-fx1iyhbhNJpNL2W72bWdK72_mRBLNX5DUDtcMfnDli-x7Ong
DDx: Includes osteomyelitis and tarsal coalition.
Tx: Rest from aggravating activities, NSAIDs, ice (both pre and post sport). When pain free a program of stretching (gastrocnemius-soleus), strengthening (dorsiflexors) and shoe inserts (heel cups, lifts, pads, or orthotics) can provide significant pain relief.
Iliotibial band syndrome (ITBS)
http://footcarexpress.com/foot-orthotics/wp-content/uploads/2009/01/iliotibial-band-syndrome.jpg
Hx -
PE-
Tx
Involves an avulsion of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx.
Ring finger is most commonly involved.
Usually occurs from a grabbing attempt (resulting in forced DIP extension during maximal FDP contraction) as would occur while attempting to grab someone’s jersey such as in football or rugby.
Clinically, there is normal passive DIP ROM with loss of active flexion. Examine this by asking the patient to flex the fingertip at the DIP while the PIP joint is held in extension.
*Remember that patients with a 90% full-thickness tendon laceration may still have normal (albeit painful) range of motion. The examiner must evaluation the strength of the tendon against resistance. This injury is commonly missed as it is diagnosed as a “jammed” finger.
Plain films may show a bony avulsion, but are often negative.
Treatment is primary repair especially with large bony fragments. Partial ruptures can be treated nonoperatively at the discretion of the hand surgeon.
Commotio Cordis
Emergency medicine & sports medicine physicians often cover sporting events where athletes are at risk of commotio cordis
Cervical Radiculopathy
The most commonly affected level is C7 (31-81%), followed by C6 (19-25%), C8 (4-12%) and C5 (2-14%)
Anterior compression can selectively affect motor fibers
Posterior compression can selectively affect sensory fibers
-More common due to posterior lateral disc herniation or facet degeneration
Signs and symptoms: Sensory complaints (findings are in a root distribution) and possible weakness and reflex changes.
Chief complaint: “Posterior heel pain”
http://www.aidmybursa.com/_img/ankle-retrocalcaneal-subcutaneous-bursitis.jpg
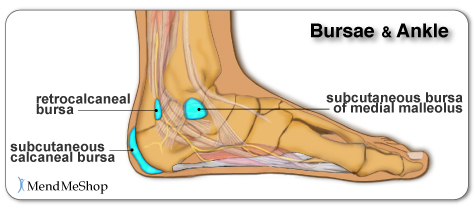
Retrocalcaneal bursitis
The retrocalcaneal bursa is located between the Achilles tendon and the posterior superior border of the calcaneus.
H&P: Inflammation and pain may follow repetitive dorsi/plantar flexion of the ankle (excessive running, jumping activities). Tenderness anterior and superior to the Achilles insertion on the heel.
Treatment: Minimize weight bearing. ½ inch elevation. NSAIDs.
Posterior calcaneal bursitis
This bursa is subcutaneous, just superficial to the insertion of the Achilles tendon.
H&P: Inflammation and pain may follow irritation from the upper border of the heel counter of a shoe. Posterior heel pain. Tender “bump” (the inflamed and swollen bursa) on the back of the heel.
http://podiatry.files.wordpress.com/2006/12/patient2.jpg
Treatment: Opened-heeled shoes, sandals, or placement of a “U-shaped” pad between the heel and the counter. NSAIDs. Advance to shoes with soft or less convex heel counters.
Transverse Myelitis
A group of inflammatory disorders characterized by acute or subacute motor weakness, sensory abnormalities and autonomic (bowel, bladder, sexual) cord dysfunction.
Symptoms are usually bilateral but both unilateral and asymmetric presentations can occur.
Look for a well-defined truncal sensory level
-below which sensation of pain and temperature is altered or lost.
Causes: Autoimmune after infection or vaccination (60% of cases in children), direct infection, or a demyelinating disease such as MS. No cause is found in 15 – 30% of cases.
Incidence: Bimodal peak at 10-19 years and at 30-39 years.
Diagnostic testing: MRI of the ENTIRE spine to both rule out structural lesions and rule in an intrinsic cord lesion. If MRI is normal reconsider the original diagnosis.
Treatment: Steroids are first-line therapy. Dosing is controversial but generally involves high IV doses for 3-5 days (1000 mg methylprednisolone). Plasma exchange is second line for those who don’t respond to steroids.
Epidural compression syndrome encompasses spinal cord compression, cauda equina syndrome, & conus medullaris syndrome.
Causes include:
Measurement of a post-void bladder residual volume tests for the presence of urinary retention with overflow incontinence (a common, though late finding) (sensitivity of 90%, specificity of 95%). Large post-void residual volumes (>100 mL) indicate a denervated bladder with resultant overflow incontinence and suggest significant neurologic compromise. The probability of cauda equina syndrome in patients without urinary retention is approximately 1 in 10,000.
Use this in your daily practice!!
The administration of glucocorticoids can minimize ongoing neurologic damage from compression & edema until definitive therapy can be initiated. The optimal initial dose and duration of therapy is controversial, with a recommended dose range of dexamethasone anywhere from 10 to 100 mg intravenously. Consider traditional dosing (dexamethasone 10 mg) for those with minimal neurologic dysfunction, & reserve the higher dose (dexamethasone 100 mg) for patients with profound or rapidly progressive symptoms, such as paraparesis or paraplegia.
Previous pearls have described tips for smart and safe documentation of typical ED complaints such as chest pain. Properly assessing and documenting orthopedic complaints is likewise very important. No evaluation or chart is complete if it does not include include the following 7 components:
The joint above
The joint below
Motor
Sensory
Vascular
Skin
Compartments
The joint above/below is important in cases of shoulder and hip pain actually being radicular pain (from the neck and back respectively). Also, hip pain from trauma may be due to a femur fracture for example.
For motor and sensory evaluation, test the most distal isolated innervation of a particular nerve (L5 - great toe dorsiflexion for example).
Note distal pulses and check ABIs for injuries with potential subtle vascular findings.
Note intact skin especially in cases where the joint will be covered by a splint.
Note "soft" compartments especially in cases of forearm and lower leg fractures.
{kind=link}
{kind=link}
{kind=link}