- When examining the hand, care should be taken to thoroughly assess both the sensory and motor function on both the dorsal and palmar surfaces.
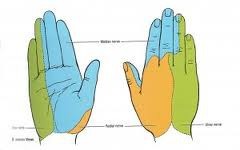
- The dermatomes of the hand provide sensation and are comprised of the ulnar, median, and radial nerves (see diagram below).
- (1) Light touch, (2) sharp touch (i.e. pinprick), (3) temperature, (4) propioception (joint position sense), (5) vibration, and (6) 2-point discrimination in the following nerve distributions should be assessed:
-- ulnar nerve >>> supplies palmar surface and dorsal tips of little finger and medial half of ring finger, including
adjacent parts of hand.
-- median nerve >>> supplies palmar and dorsal aspects of thumb, index finger, middle finger, and lateral half
of ring finger, including adjacent parts of hand.
-- radial nerve >>> supplies most of dorsal surface of hand.